
HMP Long Lartin
Report on an announced inspection of HMP Long Lartin by HM Chief Inspector of Prisons 15 February–5 March 2026.

Introduction (Back to top)
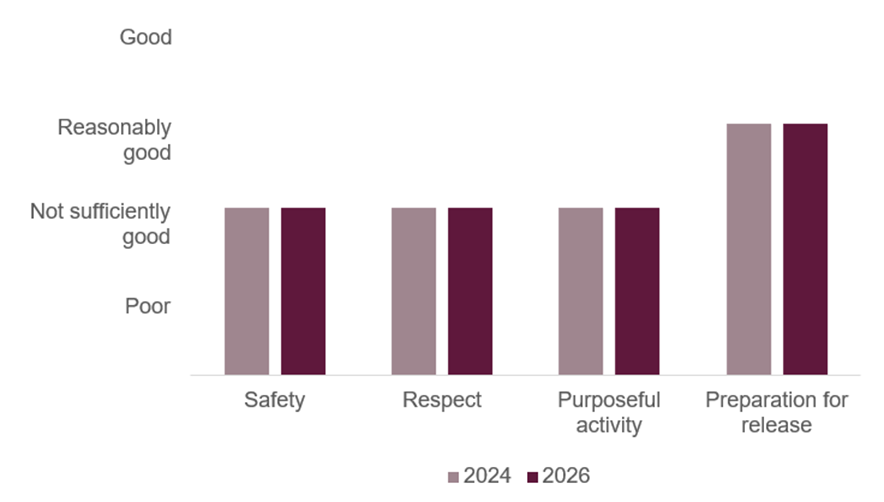
HMP Long Lartin, a high security prison near Evesham in Worcestershire, holds some of the more dangerous men in the country, the majority presenting a very high risk of harm and serving long or indeterminate sentences. This creates a demanding environment in which to deliver safe custody, decent treatment and genuine opportunities for progression. We last inspected the prison in 2024 when outcomes for those detained were insufficient in three of our four tests of a healthy prison. Only in preparation for release were outcomes assessed as reasonably good. At this announced follow up inspection, we found a well led prison which was making progress, but outcomes for prisoners had not improved enough to change the scores in any of our tests.
Many prisoners told us they felt unsafe. Violence remained prevalent, although the rate of assaults had begun to fall. Four more prisoners had taken their own lives since our last visit and the rate of self‑harm remained high. Systems to manage risk were too often weak or applied inconsistently and we found too few meaningful interventions for those who were distressed, isolated or disengaged. While there had been some improvements in the governance of use of force, overall levels remained the highest amongst comparable prisons. Leaders had, however, been successful in reducing the supply of illicit drugs through a combination of methods, a notable achievement reflected in a steep drop in positive mandatory drug tests.
Too many prisoners lived in unacceptable conditions. On older wings, men still relied on the demeaning night-sanitation system, and on other wings many cells lacked heating or hot water. These problems are long‑standing and will not be resolved without substantial and sustained investment. Leaders had worked hard to improve cleanliness in communal areas, but the daily experience for many prisoners was characterised by a lack of support and frustration. Staff–prisoner relationships were fragile. We saw some positive interactions, but too many staff failed to engage confidently or constructively with prisoners, whilst work to promote equality and inclusion remained inconsistent.
Prisoners spent long periods locked in their cells, particularly at weekends, with limited access to work, education or meaningful association. A significant number of men were allocated to full‑time activity, but frequent cancellations meant that many were only occupied intermittently. Some areas of provision were better – the gym and library offered good resources when prisoners could attend, and outreach education helped a small number of men who would otherwise have been excluded – but overall, there were too few activity places and too little ambition in what was provided.
The offender management unit was well led and fully staffed, and many prisoners had regular contact with experienced prison offender managers. Public protection arrangements were effective, and work with young adults had improved significantly. However, even in this area, leaders did not make best use of data to identify gaps in provision or to prioritise risk‑reduction work. Many prisoners had too few opportunities to demonstrate progression, particularly those seeking recategorization or access to accredited offending behaviour programmes.
Since the last inspection, the governor had set clear standards for improvement, some of which were being achieved and there was evidence of greater stability. Staff supported his approach, but morale was low and shortages of experienced officers had weakened delivery. Leaders had achieved a reasonable level of control over security, including notable success in reducing drug supply, but overall progress needed to speed up. Too many of our previous concerns had not been addressed, and several remained priorities.
Charlie Taylor, HM Chief Inspector of Prisons, April 2026
Outcomes for prisoners (Back to top)
We assess outcomes for prisoners against four healthy prison tests: safety, respect, purposeful activity, and preparation for release (see More about this report for more information about the tests). We also include a commentary on leadership in the prison (see Section 1).
At this inspection of HMP Long Lartin we found that outcomes for prisoners were:
- Not sufficiently good for safety
- Not sufficiently good for respect
- Not sufficiently good for purposeful activity
- Reasonably good for preparation for release.
We last inspected HMP Long Lartin in 2024. Figure 1 shows how outcomes for prisoners have changed since the last inspection.
Figure 1: HMP Long Lartin healthy prison outcomes 2024 and 2026
What needs to improve (Back to top)
During this inspection we identified 15 key concerns, of which five should be treated as priorities. Priority concerns are those that are most important to improving outcomes for prisoners. They require immediate attention by leaders and managers.
| Priority concerns | |
| 1. | The rate of assaults was higher than at similar prisons, and leaders had not done enough to understand the underlying causes of violence. |
| 2. | There had been four self-inflicted deaths since the last inspection, and the rate of self-harm incidents was higher than at similar prisons. Support for prisoners in crisis was poor. |
| 3. | Many staff failed to engage positively with prisoners, and minority ethnic prisoners reported especially poor relationships with staff. |
| 4. | The unhygienic night sanitation system was still in use and many prisoners did not have heating or hot water. These serious issues could not be resolved without substantial and sustained investment. |
| 5. | Attendance at workshops was poor. |
| Key concerns | |
| 6. | Force was used more frequently than in similar prisons and its governance was weak. |
| 7. | Many prisoners complained about the quality of the food. The main kitchen remained closed, limiting the range of meals that could be provided. |
| 8. | Work to support fair treatment and inclusion was inconsistent and poorly coordinated. Senior leaders lacked drive and focus on this area and significant concerns were not being addressed. |
| 9. | The poor condition of the health centre posed risks to patients’ health and well-being. |
| 10. | Patients waited too long for transfer to hospital under the Mental Health Act. One unwell man had waited for 277 days at the time of the inspection. |
| 11. | Prisoners still had too little time out of cell, especially at the weekends. |
| 12. | Leaders had not ensured sufficient spaces for prisoners to engage in full-time purposeful activity. |
| 13. | The quality of education that prisoners received in workshops was not of a consistently high standard. |
| 14. | Family work had deteriorated significantly. Over half the population had not received a social visit in the past year and most of the work to support them had ceased. |
| 15. | Prisoners did not have enough opportunities to complete the risk reduction work that could help them to progress through sentence. |
Notable positive practice (Back to top)
We define notable positive practice as evidence of our expectations being met to deliver particularly good outcomes for prisoners, and/or particularly original or creative approaches to problem solving. Inspectors found five examples of notable positive practice during this inspection, which other prisons may be able to learn from or replicate.
| 1. | The foreign national specialist had improved the prison’s understanding of these prisoners’ needs. (See Fair treatment and inclusion.) |
| 2. | The library and gym delivered innovative enrichment activities, including trauma-informed yoga, a chess competition and an accredited course for young adults. (See Time out of cell.) |
| 3. | An outreach tutor provided in-cell education, including to segregated and self-isolating prisoners and those struggling to engage with standard education classes. (See Segregation and Education, skills and work activities.) |
| 4. | The chaplaincy’s ‘Keeping in Touch’ initiative helped prisoners with neurodiverse needs and those with low literacy or numeracy to re-establish relationships with family members. (See Children and families and contact with the outside world.) |
| 5. | Work with young adults had improved significantly with regular, well-attended consultation forums with young prisoners, and the appointment of dedicated staff in several departments, including the Offender Management Unit and Psychology. (See Reducing reoffending.) |
Unless otherwise specified, these examples are not formally evaluated, are a snapshot in time and may not be suitable for other establishments. They show some of the ways our expectations might be met, but are by no means the only way.
Section 1: Leadership (Back to top)
Leaders provide the direction, encouragement and resources to enable good outcomes for prisoners.
The governor had continued to set clear standards and promote accountability and professionalism among staff. Many staff told us they supported his approach and that the prison had progressed. However, they also reported low morale, shortages of experienced officers, and concerns about staffing levels. A serious assault on an officer the previous summer had shaken the confidence of frontline staff, and leaders believed it had contributed to subsequent departures and weakened staff-prisoner relationships. Some proactive custodial managers had made efforts to build a more positive staff culture, but this was not a consistent approach across all wings.
The security team was cohesive, well led and had taken robust and successful action to tackle the threat of illicit drugs. Leaders had also strengthened physical security, investing in anti-drone wires and temporarily closing a wing vulnerable to drone incursions.
Leaders had achieved a reasonable level of control and good order, but there had been insufficient work to understand the underlying causes of violence and self-harm.
Serious infrastructure problems persisted and could not be resolved without substantial and sustained investment. Leaders had still not replaced the outdated night sanitation system (see Glossary); the governor had submitted a bid for in-cell toilets and sinks after the previous inspection. Efforts by leaders to address the poor performance of the facilities management provider had not been effective, and the significant disrepair continued to impact on prisoners’ daily lives.
More positively, energetic work by the heads of residence had strengthened prisoner consultation and improved cleanliness in outdoor communal areas.
Leaders had been proactive in addressing concerns about the culture in the segregation unit. The unit was now well led and there was early evidence that it was providing more reliable and professional care to some very challenging prisoners.
A committed equality team had begun to make progress in supporting prisoners, but the approach from senior leaders was not strong enough to embed an inclusive culture across the establishment.
The health care department was well led, but partnership working remained inadequate, and longstanding poor conditions in the health care centre had still not been resolved.
Leaders had prioritised improvements to the regime, and education provision was generally good. However, despite some strong work by the head of education, skills and work, there were too few full-time activity places and the quality of teaching in two workshops was poor.
Inconsistent leadership and the absence of PACT (Prison Advice and Care Trust) staff had contributed to a decline in family services, and leaders did not sufficiently recognise the importance of this work to safety and well-being.
The offender management unit was well led, fully staffed and reasonably effective, but there was insufficient strategic focus on individual risk reduction work that could support recategorisation.
Across the prison, data were not analysed or used effectively enough to drive improvement.
Section 2: Safety (Back to top)
Prisoners, particularly the most vulnerable, are held safely.
Early days in custody
Expected outcomes: Prisoners transferring to and from the prison are safe and treated decently. On arrival prisoners are safe and treated with respect. Risks are identified and addressed at reception. Prisoners are supported on their first night. Induction is comprehensive.
An average of three prisoners a week arrived at Long Lartin. A peer worker was available to support new arrivals. Routine body scanning of new arrivals led to regular finds of contraband. All men were strip searched in addition, but there was no information or data as to the efficacy of this measure. Prisoners still experienced delays in receiving their property.

Reception staff completed an appropriate risk and safety interview, but it did not take place in a private office, potentially inhibiting disclosure. Prisoners arriving in the evening were often not assessed until the following day.
First night areas were clean and cells were equipped with basic items. A peer worker helped new arrivals settle on the unit, and wing, safety and chaplaincy staff carried out further private interviews. Staff completed appropriate first night checks. If prisoners could not access their telephone accounts, staff contacted their families to say they had arrived.

The induction process covered key information but took too long, with many prisoners waiting three weeks or longer, instead of the scheduled two weeks, to complete all elements. This delayed their allocation to activity and meant they spent extended periods on the wing with little to occupy them
Promoting positive behaviour
Expected outcomes: Prisoners live in a safe, well ordered and motivational environment where their positive behaviour is promoted and rewarded. Unacceptable conduct is dealt with in an objective, fair, proportionate and consistent manner.
Encouraging positive behaviour
| Data provided by the prison | |
| Rate of prisoner-on-prisoner assaults per 1,000 prisoners in the 12 months to the end of February 2026 | 185 |
| Rate of prisoner-on-staff assaults per 1,000 prisoners in the 12 months to the end of February 2026 | 214 |
The rate of assaults had been falling, but it was still the second highest for the type of prison. The number of serious assaults in the last year – 15 on prisoners and 11 on staff – was also comparatively high. In our survey, 39% of prisoners said they felt unsafe at the time of the inspection.
Leaders did not have enough understanding of the underlying causes of violence, and only a minority of surveyed prisoners said they would report bullying or victimisation from other prisoners (32%) or staff (39%). More than 100 challenge, support and intervention plans (CSIPs, see Glossary) had been opened in the previous year, but they had limited value in understanding the drivers of violence: many investigations were inadequate and plans were often blank.
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Do you think the culture within this prison encourages prisoners to behave well? | 6% | Lower |
The prison did not promote positive behaviour well enough. Only 8% of prisoners in our survey said that good behaviour was rewarded fairly, and records did not always provide a clear rationale for keeping prisoners on the basic level of the incentives scheme. Some had been at this level for over three months and reviews were not always timely.
Ten prisoners were self-isolating during the inspection, including some for more than a year. Support for these individuals had been very limited. Multidisciplinary reviews had recently started but it was too soon to judge if these were significantly improving provision.
The backlog of adjourned adjudications had reduced from over 100 at the last inspection to around 55. Assurance and oversight to manage police referrals and adjourned adjudications were now good. Hearings were conducted well, and community payback awards had been used seven times in the last year, which was low but more than we often see. However, adjudications standardisation meetings did not routinely generate actions, assess consistency or identify overuse.
Use of force
| Data provided by the prison | |
| Annual rate of use of force incidents per 1,000 prisoners to end of February 2026 | 1,080 |
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Have you been restrained by staff in this prison in the last six months? | 35% | Higher |
Use of force was higher than at the last inspection, and when compared to similar prisons. However, it had been reducing in the previous six months and there had been a notable drop in the most serious interventions in the previous year. There had been less use of PAVA incapacitant spray, drawn on 16 occasions and deployed on seven of these occasions. Batons had not been used at all and special accommodation used just once. All incidents were now investigated and documented appropriately.
Body-worn camera footage was available for 78% of incidents, which was better than in most other high security prisons. However, in many cases only one camera had been activated, and some recordings did not capture the full event. Footage showed mainly adequate management of situations, but we saw some poor behaviour that had not been identified by leaders. A weekly scrutiny meeting reviewed all incidents, but operational leaders did not always attend.
The monthly use of force meeting considered a range of data, but trend analysis was weak and concerns were not addressed promptly. For example, 55% of incidents in the year to the end of February 2026 involved prisoners with disabilities, but there had been no work to understand or reduce this above-expected level of force.
Segregation
| Data provided by the prison | |
| Average number of prisoners held in segregation each month in the 12 months to the end of February 2026 | 39 |
| Average length of segregation in the unit in days in the 12 months to the end of February 2026 | 39 |
Leaders had identified some poor staff behaviour and attitudes in the segregation unit, and this was reflected in our survey, where only 17% of prisoners who had been segregated in the previous six months said they had been treated well by staff. A new head of function had been appointed to improve the management and culture of the unit, and there was some evidence of positive early outcomes. Most of the segregated prisoners we spoke to during the inspection spoke appreciatively about the support they were currently receiving from staff and we observed respectful and professional staff-prisoner interactions.
The average length of stay in the unit was high but had reduced since the last inspection, from 61 to 39 days. Staff had detailed knowledge of some complex and challenging prisoners and had undertaken good work to reintegrate or transfer them to other establishments. These actions were not always well documented, and support plans were generic.
The environment had been improved through investment in flooring and repainted cells, but exercise yards remained stark, showers lacked ventilation and nearly half of in-cell phones were broken. The regime was limited to daily exercise, a phone call and a shower, but it was positive that about half of segregated prisoners received education through an outreach tutor.
A segregation, monitoring and review group met quarterly and considered a range of data, but there had been little resulting action to drive improvement.


Security
Expected outcomes: Security and good order are maintained through an attention to physical and procedural matters, including effective security intelligence and positive staff-prisoner relationships. Prisoners are safe from exposure to substance misuse and effective drug supply reduction measures are in place.
Leaders had a good understanding of key security threats. There was a high level of intelligence reporting, with no processing backlogs. Information was shared appropriately with relevant prison departments and external agencies. Security, safety and residence leaders met weekly to share information and identify actions.
| Data provided by the prison | |
| Random mandatory drug test positive rate in the 12 months to the end of February 2026 | 8% |
The mandatory drug testing (MDT) positive rate had fallen steeply since the previous inspection, from 27% to 8%. This had been achieved through a range of measures, including installation of drone prevention wires, a strong response to staff corruption, and the closure for refurbishment of a wing identified as a drone hotspot.
The drug strategy was up to date, and key leaders attended monthly meetings to help coordinate actions. A comprehensive action plan set out clear priorities to reduce drug supply and demand, and there was strong support for prisoners with substance misuse needs (See Mental health and substance use).
New window grilles were being installed to further reduce opportunities for prisoners to pass or receive illicit items. The main remaining weakness was that only 56 of the 240 suspicion drug tests requested in the previous year had been completed, reducing their deterrent effect.


Searching procedures and review processes were up to date and there was appropriate oversight of category A, escape list and Terrorism Act (TACT) prisoners.
Safeguarding
Expected outcomes: The prison provides a safe environment which reduces the risk of self-harm and suicide. Prisoners at risk of self-harm or suicide are identified and given appropriate care and support. All vulnerable adults are identified, protected from harm and neglect and receive effective care and support.
Suicide and self-harm prevention
| Data provided by the prison | |
| Rate of self-harm per 1,000 prisoners in the 12 months to end of February 2026. | 858 |
There had been four self-inflicted deaths since the previous inspection, more than at similar prisons. There had been relatively few recommendations from subsequent death in custody reports, so it was particularly disappointing that some had not been addressed. These included weak support for those at risk of self-harm (see below) and removing blocked observation panels. During our night visit, we also observed weak staff handovers for those at risk of self-harm, and not all staff carried anti-ligature knives.
The rate of self-harm had fallen by 31% since the last inspection but remained higher than in similar prisons. Although the monthly safety meeting considered a range of data, actions were inadequate. For example, the incentives scheme and adjudications had been identified as factors that might contribute to self-harm, there had been little work to understand why. Actions from the weekly safety intervention meeting were also not always completed promptly.
All wings now had Listeners (prisoners trained by the Samaritans to provide confidential emotional support to fellow prisoners) and access to them was generally reasonable. However, several told us that some staff did not understand their role and there was evidence that they were not given access to wings to provide follow-up support.
Records of assessment, care in custody and teamwork (ACCT) case management for prisoners at risk of suicide or self-harm showed inconsistency and weak daily oversight, with few recorded observations and conversations. In some cases, there had been no review after an escalation in risk. There were few interventions to support individuals who were low in mood or in crisis. We spoke to several prisoners on ACCT who did not feel well supported.
Protection of adults at risk (see Glossary)
Wing staff had little awareness of how and when to raise safeguarding concerns, and most referrals came from health care staff (see Social care section). The safety intervention meeting discussed some relevant cases, but there was no evidence of actions or monitoring of outcomes.
Section 3: Respect (Back to top)
Prisoners are treated with respect for their human dignity.
Staff/prisoner relationships
Expected outcomes: Prisoners are treated with respect by staff throughout their time in custody and are encouraged to take responsibility for their own actions and decisions.
| HMIP prisoner survey | Yes | Compared with similar prisons | Compared with last inspection |
| Do most staff here treat you with respect? | 53% | Lower | Lower |
Some staff engaged positively with prisoners, but too many stayed together in groups instead of interacting with prisoners. Many men, especially those from some minority groups (see Fair treatment and inclusion section), told us they wanted a change in staff approach:
‘… Staff that care and know how to talk to other adults, to understand that at one time or another we were out there as regular citizens…’
Prisoners and staff alike told us that the lack of experience of many staff and frustration caused by a lack of activity (see Purposeful activity section) undermined relationships. Leaders also told us that a serious assault on an officer the previous summer had affected staff confidence (see Encouraging positive behaviour section).
Key workers (see Glossary) were allocated to all prisoners, and managers were pushing hard to drive improvement in the quality and quantity of this work. However, few prisoners told us that they had regular key work, and records showed that most were not receiving monthly sessions. The sessions generally did not actively support prisoners to progress through their sentence.
Daily life
Expected outcomes: Prisoners live in a clean and decent environment and are aware of the rules and routines of the prison. They are provided with essential basic services, are consulted regularly and can apply for additional services and assistance. The complaints and redress processes are efficient and fair.
Living conditions
Communal areas were in much better condition than at the last inspection, especially external areas. We no longer saw litter and rubbish bags lying around the site.

Flooring in the older wings had been replaced, but there were still many problems with the condition of the prison and essential equipment. Many wing areas were still grubby with ingrained dirt, although residential managers had worked hard to improve day-to-day cleanliness.
One wing had not had hot water for months, which was unacceptable and taking far too long to resolve. Many shower rooms were in poor condition through lack of ventilation. The self-cook areas were also shabby with broken equipment, although replacements were due to be installed soon. Laundry rooms were similarly run down.

Prisoners on the older wings, with no running water in the cells, still had to use the unpopular night sanitation system (see Glossary). Although managers had taken steps such as providing rudimentary camping toilets rather than buckets in the cells, the system remained demeaning.
Leaders had reduced the amount of prisoner property clogging up the reception area and had improved prisoner access, but they still had many justified complaints about delays in accessing their personal property.

We saw staff ignore cell call bells for considerable periods, and this was reflected in the prison’s electronic records and our survey, where only 18% of prisoners said bells were normally answered within five minutes.
Residential services
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Is the quality of the food in this prison very/quite good? | 21% | Lower |
The main kitchen had been closed for 19 months. A larger temporary kitchen had replaced the completely inadequate one in use at the previous inspection, and the temporary catering manager had made some recent improvements to the quality of food in response to prisoner forums. Despite this, the range of food provided was still limited and elicited many complaints. For example, in our survey only 8% of Muslim respondents said the food was good.
Prisoners were also less satisfied than the comparators with the range of purchases they could make, including catalogue orders. The service from suppliers had not always been reliable.
Prisoner consultation, applications and redress
| HMIP prisoner survey | Yes | Compared with the last inspection |
| Are prisoners here consulted about things like food, canteen or wing issues? | 63% | Higher |
| If so, do things sometimes change? | 26% | Higher |
Consultation with prisoners had improved and was now good. The well-attended prison council meetings covered more issues than in many establishments, and progress was tracked well from meeting to meeting. Many concerns were addressed reasonably promptly, but physical repairs and replacements were often delayed. There was also a range of wing consultation forums.
Prisoners still had to make applications on paper forms, but the timeliness of responses was tracked and analysed well. The complaints system was also administered efficiently, and responses were quality checked with feedback to managers where necessary. However, in our survey, only 18% of those who had made a complaint and 37% of those who had made an application said they were dealt with fairly. Leaders had little insight into the reasons for these negative responses.
Many prisoners were unhappy with their access to legal advisers: contact by phone was difficult as the in-cell phones were turned off for most of the working day, and in-person legal visits were now allowed only in exceptional circumstances – this was an excessive restriction, although leaders were not applying the criteria rigidly during the inspection. Prisoners had access to current legal texts, and the confidentiality of legal mail was respected.
Fair treatment and inclusion
Expected outcomes: There is a clear approach to promoting equality of opportunity, eliminating unlawful discrimination and fostering good relationships. The distinct needs of prisoners with particular protected characteristics (see Glossary) or those who may be at risk of discrimination or unequal treatment, are recognised and addressed. Prisoners are able to practise their religion. The chaplaincy plays a full part in prison life and contributes to prisoners’ overall care, support and rehabilitation.
Work to support fair treatment and inclusion was inconsistent and poorly coordinated, and there had been little progress in developing a more inclusive culture since the last inspection.
For example, in our survey, more minority ethnic prisoners (64% compared to 39% of white men) and prisoners with a disability (66% compared to 38% of those without) reported bullying or victimisation by staff (see also Use of force section). Leaders had limited understanding of such findings.
We found evidence of poor staff attitudes towards some prisoners with disabilities, and some with mobility problems were unable to access the education, chapel and health care.
Approximately 12% of discrimination incident reporting forms (DIRFs) submitted in 2025 were fully or partially upheld. Investigations were generally of good quality, and the Zahid Mubarek Trust (ZMT), the governor and ZMT equality advocates provided effective scrutiny. Some cases resulted in tangible actions, such as the production of easy-read resources following a complaint from a prisoner with learning difficulties. However, poor tracking meant it was unclear what had been addressed, and DIRF responses were not prompt.
There had been little action following equality meetings to address identified disproportionality. A committed equality adviser had worked hard to raise the profile and effectiveness of the work but had lacked management support until recently. However, there was some positive work with specific groups, including impressive work with young adults (see section on Reducing reoffending). There was also emerging but more piecemeal work with neurodiverse men, who benefited from a recently established neurodiversity support panel (which identified support for complex cases), and easy-read resources. The foreign national officer had delivered training to staff and distributed a useful monthly newsletter.
Faith and religion
The chaplaincy provided a range of support to prisoners and had strong links to other departments, including safety and security. In our survey, 93% of respondents said they had spoken to the chaplaincy, higher than at similar prisons.
The chaplaincy delivered helpful family and substance misuse support, as well as ‘Sing Inside’ workshops, which aimed to build confidence and a sense of community. Water damage to the chapel had continued to worsen despite some repair efforts.


Health, well-being and social care
Expected outcomes: Patients are cared for by services that assess and meet their health, social care and substance use needs and promote continuity of care on release. The standard of provision is similar to that which patients could expect to receive elsewhere in the community.
The inspection of health services was jointly undertaken by the Care Quality Commission (CQC) and HM Inspectorate of Prisons under a memorandum of understanding agreement between the agencies. The CQC found a breach of regulations and issued a request for an action plan following the inspection (see CQC appendix).
Strategy, clinical governance and partnerships
Oversight of health care delivery, record-keeping and care planning had improved, and patients now received timely, person-centred care. Regular bespoke clinical audits had contributed to improvements. We saw learning from adverse incidents, complaints and patient feedback, which had enhanced service delivery.
The service was well led, and effective recruitment had increased staff levels. Health staff received regular supervision and were mostly compliant with mandatory training. We observed kind and professional interactions between staff and patients.
Strategic partnership working had made limited progress on several long-standing environmental deficits, which posed risk to patients’ health and well-being (see Primary care section).
The risk register held by the provider Practice Plus Group (PPG) had not identified the limited psychiatry staffing to meet the needs of the population or the inadequate space to deliver some services.
Local concerns and complaints were dealt with effectively, but there had been long delays in responses from the national PPG team; however, this had now been resolved.
Promoting health and well-being
An enthusiastic and active patient engagement lead officer used every opportunity to promote health, including a range of health events. Health champions on each wing delivered health and well-being events, were committed and well supported, and said they enjoyed their role.
Prisoners could access NHS health checks, national screening programmes and blood-borne virus screening. Work was under way to increase uptake, including staff training.
There was an in-house sexual health service and good working relationships with secondary care specialists. Patients could access this help confidentially, but records were not stored in a standalone confidential system.
Primary care and inpatient services
Patients requested appointments through a well-managed, paper-based system, with all applications clinically triaged. Urgent care was accessible within one day and routine GP appointments within three weeks, which was comparable with the community. Patients had access to a range of appropriate allied health professionals, with reasonable waiting times.
New arrivals received an initial health screening to identify immediate needs, followed by a second screening within required timescales.
Patients with long-term health conditions now had effective oversight, and their health monitoring and personalised care plans were completed.
Emergency medicines and equipment were accessible to staff but monitoring had not identified that some items were stored incorrectly or past their expiry date.
Administrative staff managed referrals, correspondence and other information efficiently. External hospital appointments were generally well managed, although officer escort shortages and late departures sometimes led to delayed or missed appointments.
The end‑of‑life suite and inpatient unit remained unfit for purpose, as identified in previous inspections. Admissions were often not aligned with the defined health care criteria, and prison leaders had no commitment to address this. The environment was unsuitable due to infection prevention and control concerns, periods without heating or hot water, a lack of communal space and a poor regime. The hoist in the palliative care suite was out of action. Patients with limited mobility could not safely access the inpatient unit or some health care clinics. Leaders had not taken remedial action to monitor and mitigate these risks effectively.
Social care
Social care arrangements between the prison and Worcestershire County Council were well established. An updated memorandum of understanding was due to be signed off.
No prisoners were receiving a social care package at the time of the inspection. When needed, assessments were prompt and external carers were used. An occupational therapist from the council provided a range of specialist equipment when required. Worcestershire liaised with other local authorities in preparation for release or transfer to promote continuity of care. Peer workers supported prisoners with lower-level social care needs, but they did not have formal training or supervision.
Health staff had submitted appropriate safeguarding referrals when prison staff had failed to offer basic support to prisoners awaiting equipment or unable to keep their cells clean (see Safeguarding section).
Mental health, and support and treatment for prisoners with addictions and those who misuse substances
Substance misuse and mental health care were provided by a single integrated service, which mostly met the needs of the population. There was good partnership working between the team and the drug strategy governor.
Two experienced psychiatrists were available two days a week, which was inadequate. It increased waiting times as some appointments were deferred because of frequent reprioritisation, prison regime issues or a lack of bookable space to see patients.
The experienced team worked flexibly to mitigate the risks associated with the lack of consulting rooms. Some trauma interventions took place in unsuitable, untherapeutic spaces such as the gym, where interruptions were inevitable. Despite a high number of prisoners with neurodiverse needs and long waits for ADHD assessment, the team did not have a learning disability nurse or speech and language therapist.
There was a single point of referral and initial triage assessments were prompt. Entries in health records ranged from reasonable to good. There was an appropriate range of psychological support and waiting times were good. Substance misuse and mental health care plans were in place and most were adhered to.
A duty worker was assigned each day and daily team meetings made sure that urgent care was allocated and emerging risks shared regularly.
Staff were committed to attending ACCT reviews but were not always told when they took place.
Complex patients were allocated a registered mental health nurse who made sure they had comprehensive care plans and risk management.
There had been 12 transfers of patients to mental health facilities in the previous 12 months, only one of which was within the recommended 28 days. One patient was still waiting for a bed after 277 days. Despite regular meetings with NHS commissioners to escalate severe delays, we saw little progress and an ongoing tolerance of multiple and unnecessary assessments for hospital beds.
Naloxone (a drug to manage substance misuse overdose) was available, and 43 prison staff had been trained in administering the nasal version.
The incentivised substance free living unit continued to provide a supportive environment to optimise recovery. Drug treatment services were highly visible, delivering regular groups and interventions. Voluntary drug tests were not sufficiently effective as they could not detect the most commonly used psychoactive substances.
Medicines optimisation and pharmacy services
Pharmacy services were well delivered by a skilled team who worked collaboratively with health care colleagues. The prescribing of medicines at risk of misuse was managed appropriately. Medicine reconciliation for new patients was completed promptly.
Many patients received their medicines in possession. Risk assessments were completed and regularly reviewed. The pharmacy technicians supported random checks and non-compliance resulted in a review. There had been good support to patients observing Ramadan to make sure they could take their medication appropriately.
Medicines administration was supported by pharmacy technicians. Identity checks were limited to the patient’s name and date of birth because identity cards were not issued. Although we observed good officer supervision of medication queues, staff and incident reports confirmed that this was not consistently the case. Prescribing, administration of medicines and non-attendance were recorded on SystmOne, the clinical IT system, and the latter was followed up.
Medicines were available when the pharmacy was closed, but records of use were incomplete. Patients could receive over-the-counter medication such as paracetamol. Advance notice was given of patients attending court or transferring, which enabled their medication to be prepared.
Medicines were supplied from an external pharmacy and generally delivered on time. Medication was transported suitably around the prison. Most medicines were appropriately labelled, but those in the emergency cupboard were not labelled for specific patients. Medicines were generally stored correctly, but drug trolleys were not chained to the wall when not in use, which posed a security risk.
Dental services and oral health
A full range of dental health services was available, with waiting times in line with those in the community. A dentist was available two days a week, and dental nurses supported each clinic, as well as an additional day of cover. The dental team was well regarded by patients.
There were arrangements for urgent treatment, and primary care staff used an agreed triage pathway effectively when a dentist was not on site.
The dental treatment room and decontamination areas were clean, and equipment was serviced and maintained appropriately. Dental staff had access to emergency medicines and equipment.
Section 4: Purposeful activity (Back to top)
Prisoners are able and expected to engage in activity that is likely to benefit them.
Time out of cell
Expected outcomes: All prisoners have sufficient time out of cell (see Glossary) and are encouraged to engage in recreational and social activities which support their well-being and promote effective rehabilitation.
There were insufficient activity spaces for the population and our checks showed that a third of prisoners were locked in their cell during the working day. While 66% of prisoners were in full-time roles, frequent workshop closures meant that they were not fully occupied (see Education, skills and work section).
Prisoners’ time out of cell remained too limited. Those in work could expect around 8.5 hours a day out of their cell on weekdays but unemployed prisoners had as little as two and a half hours. Weekends were worse as a ‘split regime’ meant that prisoners in half the residential units were unlocked only for the morning and the other half for the afternoon, leaving little or no time for many to complete domestic tasks.
| HMIP prisoner survey | Yes | Compared with similar prisons |
| At the weekend, are you able to complete domestic tasks? | 67% | Lower |
Apart from gym equipment (see below), there were few social or recreational activities on the wings during unlock periods, and many prisoners told us they had little to occupy them.
The library provided a good resource for prisoners when they were able to attend, but sessions were regularly cancelled – 20% in the previous month (February 2026). We were told this was because of insufficient staff to escort prisoners.
The library contained a wide range of books, including dyslexia-friendly and easy-read materials. Library staff promoted literacy well through workshop libraries, a Gatehouse (new readers) reading group, Shannon Trust literacy mentors, a book club and a creative writing course.

Prisoners spoke positively about the gym, which included a large sports hall and outdoor space. It offered a range of activities and qualifications, including creative activities such as trauma-informed yoga, an accredited PE course for young adults and a chess competition.
Attendance had been affected by some regime conflicts, but leaders assured us that this was being addressed. Gym equipment was now available on all wings, and work had begun to replace older machines.



Education, skills and work activities
Ofsted inspects the provision of education, skills and work in custodial establishments in England. The following summary has been provided by Ofsted inspectors who attended this inspection. Their full report is published under ‘Further resources’.
Ofsted made the following assessments about the education, skills and work provision:
- Overall effectiveness: Requires improvement
- Quality of education: Requires improvement
- Behaviour and attitudes: Requires improvement
- Personal development: Requires improvement
- Leadership and management: Requires improvement
Since the previous inspection, leaders had made progress in rectifying two of the three recommendations. Waiting lists for English and mathematics had been substantially reduced. Workshops that had previously been mundane were improved by introducing new activities, such as barbering and textiles. However, attendance at workshops remained weak.
Leaders had not ensured that sufficient activity spaces were available for prisoners. In several workshops, there was not enough work to keep prisoners productively occupied. Two workshops were sometimes closed due to staffing shortages, limiting prisoners’ opportunities for meaningful engagement.
Leaders had implemented a curriculum that was too narrow. They focused appropriately on preparing prisoners for careers in custody and helping them adapt to prison life. However, they had not established an ESOL curriculum or provided a dedicated tutor for prisoners who spoke English as a second language. Substantial budget reductions had limited the range of learning and work opportunities available.
Leaders in education and outreach had provided a high standard of education. However, in a small number of workshops, there was insufficient work to sustain prisoners’ engagement. Instructors lacked the necessary education and training to support effective learning, leading to low motivation among prisoners.
Leaders had introduced an appropriate reading strategy that promoted reading across the establishment. Prisoners’ literacy was assessed quickly, and reading skills were developed through a range of initiatives, including English lessons and one‑to‑one phonics support for weaker readers.
Instructors did not consistently develop prisoners’ employability skills. In workshops, prisoners monitored their early progress by completing their ‘progress in work’ workbook. However, wing workers and prisoners in longer‑term job roles were not routinely encouraged to move into alternative work or to develop additional skills.
Tutors had provided effective support for prisoners with special educational needs and disabilities. Rapid screeners were used successfully, followed by detailed, individualised assessments of need. Appropriate support plans were in place, and the curriculum was adapted well for in‑cell learning.
About three-quarters of prisoners had achieved the qualification for which they had studied. Leaders had recently implemented a new induction process to ensure that prisoners received education, skills and work induction promptly on arrival. Initial assessments and careers education, information, advice and guidance were carried out swiftly, enabling staff to identify prisoners’ starting points and direct them to next steps. However, a small number of prisoners were still awaiting review appointments due to historic delays.
Attendance and punctuality at education sessions were mostly appropriate. When prisoners attended workshops, they generally arrived on time. However, workshop attendance overall was poor. Around half of the workshops had been closed due to staff shortages, and attendance in those that remained open was 63%.
Leaders provided a broader curriculum to support prisoners’ well-being and help them settle into prison life. Enrichment activities included art, tapestry, and creative writing groups. Health initiatives such as yoga, gym sessions, and health‑champion roles helped prisoners learn about topics like diet and nutrition. However, many prisoners in the workshop did not routinely learn about topics such as respect, equality, diversity, or protected characteristics.
Section 5: Preparation for release (Back to top)
Preparation for release is understood as a core function of the prison. Prisoners are supported to maintain and develop relationships with their family and friends. Prisoners are helped to reduce their likelihood of reoffending and their risk of harm is managed effectively. Prisoners are prepared for their release back into the community.
Children and families and contact with the outside world
Expected outcomes: The prison understands the importance of family ties to resettlement and reducing the risk of reoffending. The prison promotes and supports prisoners’ contact with their families and friends. Programmes aimed at developing parenting and relationship skills are facilitated by the prison. Prisoners not receiving visits are supported in other ways to establish or maintain family support.
Family work had deteriorated. Frequent changes in leadership had undermined progress, and there was too little focus on the broader role of families in promoting safety and reduced reoffending.
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Have staff here encouraged you to keep in touch with your family/friends? | 24% | Lower |
Social visits were the main focus of family provision and were well managed. The in-house booking system was effective, with a direct number to a dedicated member of staff. However, there were some long delays in completing visitor checks for category A prisoners.
Staff worked hard to create a relaxed and child-friendly environment in the visits hall, including in the separate room used for high-risk category A prisoners. There was enough space and most families and friends we spoke to were positive about their visits experience. Some hot food had recently been introduced, catering for different dietary requirements.

Over half the population had not received a social visit in the past year, including 73 men who had never had one. Official prison visitors saw a few prisoners but the extensive work to support these prisoners that we saw at the last inspection had ceased. Although PACT (Prison Advice and Care Trust) was funded to provide casework and support for these prisoners, they had not had the staff to do this.
This was partly mitigated by the chaplaincy’s ‘Keeping in Touch’ sessions, which helped prisoners who had lost contact with their families to reconnect. Chaplains supported prisoners with neurodiverse needs and/or low literacy and numeracy skills with letter writing and how to have a good social visit. There had been four of these sessions so far, each attended by seven to 10 prisoners.
Regular structured six-hour family visits were valued by prisoners and their families. Following a recommendation from the prison’s young adults’ forum, adult family members were also eligible to attend. However, prisoners convicted of sexual offences had no access to family visits, and neither did anyone with a negative warning in the previous three months.
In our survey, only 10% of prisoners compared to 25% in similar establishments said they were able to use social video calls (see Glossary). Slots were only 30 minutes long, with no evening availability.
New prisoners had delays in receiving their telephone PINs, including for legal representatives. Phone calls were restricted to one hour a day, during set times, and prisoners often had to choose between contacting legal representatives or family. Other systems, such as email-a-prisoner, generally worked well.
Uptake of Storybook Dads (where prisoners record a story for their children) was low, and the process for getting recordings to children was slow.
Reducing reoffending
Expected outcomes: Prisoners are helped to change behaviours that contribute to offending. Staff help prisoners to demonstrate their progress.
| Data provided by the prison | |
| Proportion of prisoners who were serving an indeterminate sentence at the time of inspection | 73% |
| Proportion of prisoners who were assessed as posing a high or very high risk of serious harm to others at the time of inspection | 88% |
Long Lartin held a complex high-risk population, and a quarter of prisoners had been held there for four years or more. Many told us that the prison did not provide enough opportunities for them to demonstrate progression through offending behaviour work, enrichment activities or full-time employment (see also sections on Opportunities to progress and Education, skills and work). In our survey, 51% of prisoners said that their experiences in the prison had made them less likely to offend in future.
Leaders did not analyse data to understand the needs of the population or identify gaps in provision across resettlement. A new head of reducing reoffending had begun to make positive changes, but it was too early to see their impact.
How staff were supporting prisoners and managing risk
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Do you have a sentence plan? | 72% | No difference |
| For those who have a sentence plan, do you know what your objectives or targets are? | 90% | No difference |
Prisoners generally had a good awareness of their sentence plans and objectives. Prison offender managers (POMs) were visible across the prison and ran a useful fortnightly drop-in session on different wings. Most prisoners had regular face-to-face meetings with their POM.
Offender management unit (OMU) staff were experienced and capable. The unit was fully staffed, and had improved its delivery to prisoners. POMs held reasonable caseloads and had more contact with prisoners than we usually see.
Some OASys (offender assessment system) assessments were not reviewed after a significant change in the prisoner’s circumstance, which meant that risk management and sentence plans were not always accurate or appropriate. Leaders had successfully reduced the OASys backlog and had effective systems to prevent this recurring.
Public protection arrangements were reasonably good. All new arrivals were screened, and decisions made on monitoring or child contact restrictions. However, although only three prisoners were monitored at the time of inspection, records showed a week-long delay in listening to their calls.
Ten prisoners were serving an imprisonment for Public Protection (IPP) sentence, and four of this group were in the segregation unit. None had previously been released and all were significantly over their sentence length tariff. Despite good support and well-established multidisciplinary meetings, some plans were too slow to advance and lacked a clear progression pathway.
Work with young adults had improved significantly, led by the head of offender management services and two dedicated POMs. The latter held regular and well-attended forums with young adults. A monthly strategic meeting also included young adult prisoner representatives and reviewed relevant data, although this did not always lead to actions when necessary. There was a gap in support for care-experienced young adults; for example, there were no links with their personal advisors in the community.
Opportunities for prisoners to progress
| Data provided by the prison | |
| Proportion of prisoners who were category A (including provisional and high risk) at the time of inspection | 33% |
| Proportion of recategorisation assessments which resulted in a downgrade of security categorisation in the 12 months to 31 January 2026 | 5% |
Recategorisation reviews were generally timely and it was positive that POMs involved prisoners in the process. However, some decisions for category A prisoners took too long – 19 were overdue at the time of the inspection. These men had too few opportunities to complete the risk reduction work needed to achieve a lower categorisation.
Although we saw many examples of POMs and key workers completing one-to-one work, collaborative working between the OMU, key workers and psychology staff was not effective enough. For example, one prisoner had completed multiple sessions with a key worker as recommended by a recategorisation review, but, a year later this work was deemed insufficient because of a lack of psychology input.
The ‘Building Choices’ accredited programme had only been delivered to a small number so far. A few prisoners convicted of sexual offences had completed structured one-to-one work, but the prison still did not offer accredited programmes to them, and they often waited long periods to transfer to a suitable establishment.
There were some non-accredited programmes, many focusing on motivation and engagement. Psychology staff delivered some good work, including support in the segregation unit and contributions to young adult provision.
The pre-PIPE (see Glossary) unit continued to provide a constructive rehabilitative environment. Prisoners there were positive about the programme and understood how they could progress towards transfer to a PIPE. Staff delivered a range of structured programmes and community-building sessions, which included cooking together. The unit had a dedicated POM and key working was delivered more effectively than in the rest of the prison.
There had been good work to improve the unit though new gym equipment and a better tended outdoor area. Ongoing building maintenance had temporarily reduced capacity to seven places for at least six months.


Returning to the community
Expected outcomes: Prisoners’ specific reintegration needs are met through good multi-agency working to maximise the likelihood of successful resettlement on release.
Long Lartin was not a resettlement prison and only seven prisoners had been released in the past year. All had suitable housing and most went to approved premises.
All releases were discussed at the monthly interdepartmental risk management meeting, but this was not always effective in ensuring robust risk management. There continued to be poor attendance from departments other than the OMU. Weaknesses in release planning included unconfirmed late approved premises referrals and poor contact between community offender managers (COMs) and prisoners. These were not always escalated to senior managers in the community when necessary.
Practical release arrangements were good, and prisoners could now get help with bank accounts, identification and Jobcentre appointments.
Section 6: About HMP Long Lartin (Back to top)
Category of the prison
Long-term high security category A and B prison for men.
Brief history
Long Lartin was built in the 1960s as a war department ordnance depot and opened as a category C prison in 1971. The infrastructure was upgraded to meet high-security conditions in 1973. An additional wing, Perrie, was opened in June 1999, and in 2009, a new purpose-built unit, Atherton, replaced older wings, increasing capacity.
Population
537 prisoners were held at the time of the inspection. There was operational capacity for 564. (Figures provided by the prison.)
- 150 new prisoners received each year (around 13 per month).
- 63 foreign national prisoners.
- 79% of prisoners from black and minority ethnic backgrounds.
- 7 prisoners released into the community in the last year.
- 115 prisoners receiving support for substance misuse.
- 18 prisoners referred for mental health assessment each month.
Short description of residential units
A – 77 vulnerable prisoners in cells without in-cell sanitation.
B – 77 vulnerable prisoners in cells without in-cell sanitation.
C – 76 cells without in-cell sanitation (currently vacant)
D – 77 prisoners in cells without in-cell sanitation.
E – modern open-plan unit for 95 prisoners.
F – modern open-plan unit for 89 prisoners.
P – incentivised substance free living unit for 42 prisoners.
Q – Perrie Red, a modern unit for 75 prisoners.
Health care inpatient unit – for seven prisoners, including one cell for end-of-life care.
Preparation psychologically informed planned environment (pre-PIPE) unit – 18 prisoners (half vacant due to building maintenance)
Care, separation and reintegration (segregation) unit – 35 cells.
Prison status (public/private)
Public
Key providers
Physical health provider: Practice Plus Group
Mental health provider: Inclusion (part of Midlands Partnership University NHS Foundation Trust)
Substance misuse treatment provider: Midlands Partnership University NHS Foundation Trust
Dental health provider: Time for Teeth
Prison education framework provider: Milton Keynes College
Escort contractor: GEOAmey
Prison group director
Hannah Lane, Long Term and High Security Estate South
Name of governor/director and date in post
Babafemi Dada, December 2023
Changes of governor/director since the last inspection
None
Date of last inspection
30 September – 10 October 2024
Progress on concerns from the last inspection (Back to top)
At our last inspection in 2024 we raised 14 concerns, five of which were about areas of priority concern.
At this inspection we found the following progress:
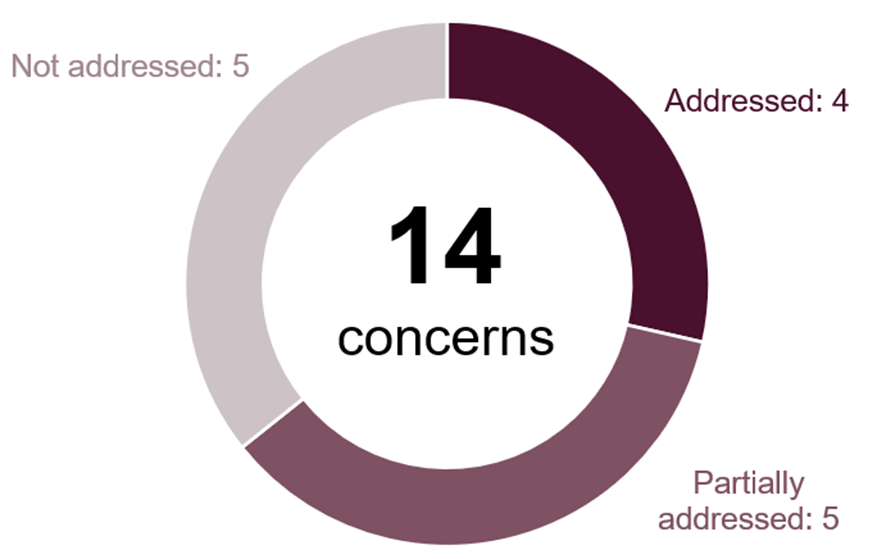
The following is a list of all the concerns raised, organised under the four tests of a healthy prison.
Safety
Priority concerns
Leaders had not done enough to understand and respond to the drivers of violence, which was too high and on an upward trend.
Not addressed
Large quantities of drugs and other illicit items were entering the prison, especially on drones. Physical security and counter measures were not robust enough, and neither national nor local leaders had addressed this longstanding problem with sufficient urgency.
Addressed
Key concerns
Early days arrangements were weak. Too many new arrivals received an abridged health screening, first night interviews were not sufficiently thorough, first night cells were not always clean or well-equipped, and induction was not delivered promptly.
Partially addressed
Self-harm had increased and leaders had not done enough to understand or respond to the reasons behind it. Governance and oversight of key areas to protect the vulnerable, such as use of constant supervision and anti-tear clothing, were weak.
Partially addressed
Respect
Priority concerns
The ‘night sanitation’ electronic rotational unlock system led to unhygienic conditions, and created opportunities for illicit activity and bullying.
Not addressed
Many wings were dirty and shabby, and large amounts of rubbish were allowed to accumulate around the prison.
Partially addressed
Key concerns
Kitchen facilities and the quality of food were poor. Catering staff were achieving commendable results in difficult circumstances, but they could not provide an appropriate range of food.
Not addressed
There was inadequate support for some minority groups. Those over 50, young adults and foreign nationals received little targeted provision, and the needs of prisoners with disabilities were not consistently well met.
Partially addressed
Governance of clinical records and health appointments was poor, creating potential risks to patient care and safety.
Addressed
Patients were not transferred to mental health hospitals promptly to receive necessary specialist treatment.
Not addressed
Purposeful activity
Priority concern
A significant proportion of the industries curriculum lacked ambition. Many prisoners completed mundane work, with little planning to help them develop new skills or move into more challenging job roles during generally long prison sentences.
Addressed
Key concerns
Many prisoners who wanted to improve their mathematics and English experienced long delays before they could start these courses.
Addressed
Prisoners’ attendance at work activities was not good enough. Regime delays led to many arriving up to half an hour late for their activities.
Not addressed
Preparation for release
Key concern
Many OASys (offender assessment system) assessments were out of date, and prisoners were not sufficiently involved in setting the sentence plan targets that were intended to reduce risk.
Partially addressed
Care Quality Commission Action Plan Request (Back to top)
Care Quality Commission (CQC) is the independent regulator of health and adult social care in England. It monitors, inspects and regulates services to make sure they meet fundamental standards of quality and safety. For information on CQC’s standards of care and the action it takes to improve services, please visit: http://www.cqc.org.uk
The inspection of health services at HMP Long Lartin was jointly undertaken by the CQC and HMI Prisons under a memorandum of understanding agreement between the agencies (see Working with partners – HM Inspectorate of Prisons (justiceinspectorates.gov.uk)). The Care Quality Commission issued a request for an action plan following this inspection.
| Breach of Regulation |
| Provider: Practice Plus Group Location: HMP Long Lartin Location ID: 1-4057556312 Regulated activities: Diagnostic and Screening Procedures, Treatment of disorder, disease or injury, Surgical procedures. |
| Regulation 17 Good governance of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014 Regulations for service providers and managers – Care Quality Commission (cqc.org.uk) 17 (1) Systems or processes must be established and operated effectively to ensure compliance with the requirements in this Part. (2) Without limiting paragraph (1), such systems or processes must enable the registered person, in particular, to— (a) assess, monitor and improve the quality and safety of the services provided in the carrying on of the regulated activity (including the quality of the experience of service users in receiving those services); (b) assess, monitor and mitigate the risks relating to the health, safety and welfare of service users and others who may be at risk which arise from the carrying on of the regulated activity; (c) maintain securely an accurate, complete and contemporaneous record in respect of each service user, including a record of the care and treatment provided to the service user and of decisions taken in relation to the care and treatment provided; (d) maintain securely such other records as are necessary to be kept in relation to— (i) persons employed in the carrying on of the regulated activity, and (ii) the management of the regulated activity; seek and act on feedback from relevant persons and other persons on the services provided in the carrying on of the regulated activity, for the purposes of continually evaluating and improving such services; (f) evaluate and improve their practice in respect of the processing of the information referred to in sub-paragraphs (a) to (e) |
| How the regulation was not being met: Systems and processes were not all effectively established or implemented to identify, assess, monitor and mitigate the risks relating to the health, safety and welfare of patients and others who may be at risk arising from the carrying on of the regulated activities. There was insufficient evidence to demonstrate that partnership working arrangements were being used to drive the improvements necessary to address long-standing environmental deficits. These included repeated failure of the heating and hot water systems, inoperable stairlift and hoist, infection prevention and control concerns, and medicines trolleys that were not safely secured to a fixed wall. There was insufficient evidence that these risks had been appropriately escalated, recorded or acted upon at a strategic level. Quality and safety of services were not consistently assessed, monitored, and improved. Assurance processes had not identified that some items in the emergency bags were past expiry date or were not stored appropriately. The provider’s risk register was not managed effectively, as all risks to patients and staff had not always been identified, recorded, assessed and mitigated. This included the limited psychiatry resources to meet the needs of the population and the lack of consultation space to deliver services. Where improvement actions had been taken, these were not always formally recorded. Systems to manage records relating to governance arrangements were not fully effective. CQC did not receive a statutory notification from the provider about an event that prevented or was likely to prevent them from carrying on regulated activity safely and in accordance with the fundamental standards of care. Between 26/12/25 and 07/01/26 the heating and hot water systems had failed for the in-patient unit and healthcare areas. The stairlift and hoist are inoperable. The impact of these environmental issues on staff and on patients who may have been more adversely affected was poorly recorded. There was insufficient evidence that the provider had put in place effective measures to reduce the risk of long‑term negative effects on people’s health and wellbeing. A secure, accurate, complete and contemporaneous record was not consistently maintained in respect of each patient, including decisions taken in relation to the care and treatment provided. Information about sexual health services was not stored on a confidential, standalone IT system, in line with national guidance. |
More about this report (Back to top)
This report outlines the priority and key concerns from the inspection and our judgements against the four healthy prison tests. Each of the following four sections contains a detailed account of our findings against our Expectations for men’s prisons.
Find out more about our Expectations and how we inspect
Find out more about priority and key concerns
Find out about notable positive practice
Findings from the survey of prisoners and a detailed description of the survey methodology are published alongside this report. Please note that we only refer to comparisons with other comparable establishments or previous inspections when these are statistically significant. The significance level is set at 0.01, which means that there is only a 1% chance that the difference in results is due to chance.
The tables in this report which provide data from HMI Prisons prisoner surveys also include comparisons with similar prisons.
| Description | What it means |
| Lower | the prison’s percentage is statistically significantly lower than the comparator: prisons with the same function type, or at the last inspection |
| Higher | the prison’s percentage is statistically significantly higher than the comparator: prisons with the same function type, or at the last inspection |
| No difference | the prison’s percentage is not statistically significantly different to the comparator: prisons with the same function type, or at the last inspection |
Inspection team
This inspection was carried out by:
| Martin Lomas Hindpal Singh Bhui Rachel Badman Martin Kettle Dawn Mauldon Alice Oddy Chelsey Pattison Esra Sari Emma Crook Samantha Moses Samantha Rasor Jasjeet Sohal Maureen Jamieson Tania Osborne Emily Hempstead Dayni Johnson Darryl Jones Bev Ramsell Martin Ward | Deputy Chief Inspector Team leader Inspector Inspector Inspector Inspector Inspector Inspector Researcher Researcher Researcher Researcher Lead health and social care inspector Health and social care inspector Care Quality Commission inspector Care Quality Commission inspector Ofsted inspector Ofsted inspector Ofsted inspector |
Find out more about the terms and abbreviations used in this report in our glossary.
Easy read summary and press notice (Back to top)
Survey material and Ofsted full report (Back to top)
The following files may not be suitable for users of assistive technology.
Request an accessible format
If you use assistive technology (such as a screen reader) and need a version of any of these documents in a more accessible format, please email media@hmiprisons.gov.uk. Please tell us what format you need. It will help us if you say what assistive technology you use.