
HMP & YOI Stoke Heath
Report on an unannounced inspection of HMP & YOI Stoke Heath by HM Chief Inspector of Prisons 23 February – 5 March 2026.

Introduction (Back to top)
Stoke Heath is a category C men’s prison in Shropshire that held 741 men at the time of this inspection. Relationships were a strength in a prison that benefitted from an experienced staff team, with many officers having worked in the jail for more than ten years. This provided a level of stability and continuity that was appreciated by prisoners.
The governor, who had been in post for a year, had begun to address some deep cultural issues in a jail that needed to reorientate back to its function as a training prison. She was aiming to get more prisoners into purposeful activity, but attendance was poor, with too many men choosing to remain on their wing rather than attend activity. Staff shortages meant that although the regime was reliably delivered, most men were only in part-time activity and too many continued to spend long periods of time locked up.
The boredom that this created was, no doubt, one of the causes of high levels of drug taking at Stoke Heath, which led inevitably to debt and violence. In random tests, nearly 30% of men tested positive for drugs. Gate security was weak, which increased the risk of illicit items entering the prison. The drug recovery wing was underpowered and while the incentivised substance free living unit (ISFL) provided a positive environment for well-behaved prisoners, it operated more like an enhanced unit, rather than an environment in which men could continue their recovery from addiction.
There were fewer assaults at Stoke Heath than its comparators. However, some prisoners were self-isolating for their own safety and high rates of self-harm showed the extent of distress amongst a significant proportion of men in the prison.
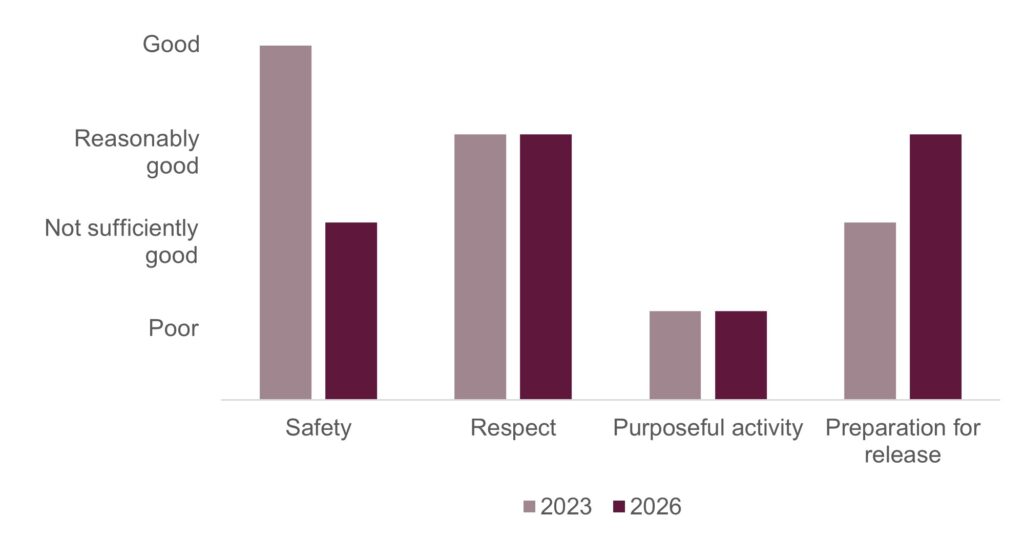
There had been an improvement in the oversight of the category D unit, Clive House, since our last inspection, and hard-working staff in the offender management unit were active in helping prisoners reduce their risk. For example, they were using more experienced POMs to support younger prisoners. Men approaching release were offered some impressive support, but the widened catchment area of the jail meant staff were having to connect with probation areas much further afield. In this area, our healthy prison test rating for preparation for release had improved from ‘not sufficiently good’ to ‘reasonably good’.
Parts of the prison were dilapidated and scruffy; E wing should be re-built, and some long-serving men were sharing small, cramped cells. However, staff made sure that the prison was kept reasonably clean, and inspectors were impressed by well-tended, litter-free grounds.
Given the remote location and the long journeys undertaken by families, it was disappointing that visits did not start on time and that family days were not long enough.
Although our rating for safety had fallen from ‘good’ to ‘not sufficiently good’ I left the jail with some optimism that if the prison can do more to improve the amount of purposeful activity and reduce the ingress of drugs, then under the positive leadership of the governor and her senior team, Stoke Heath can flourish.
Charlie Taylor, HM Chief Inspector of Prisons, April 2026
Outcomes for prisoners (Back to top)
We assess outcomes for prisoners against four healthy prison tests: safety, respect, purposeful activity, and preparation for release (see More about this report for more information about the tests). We also include a commentary on leadership in the prison (see Section 1).
At this inspection of HMP & YOI Stoke Heath, we found that outcomes for prisoners were:
- not sufficiently good for safety
- reasonably good for respect
- poor for purposeful activity
- reasonably good for preparation for release.
We last inspected HMP & YOI Stoke Heath in 2023. Figure 1 shows how outcomes for prisoners have changed since the last inspection.
Figure 1: HMP & YOI Stoke Heath healthy prison outcomes 2023 and 2026
What needs to improve (Back to top)
During this inspection we identified 12 key concerns, of which six should be treated as priorities. Priority concerns are those that are most important to improving outcomes for prisoners. They require immediate attention by leaders and managers.
| Priority concerns | |
| 1. | Drugs, particularly psychoactive substances, were too freely available. |
| 2. | Rates of recorded self-harm were very high. There was not enough prison-wide work to address the reasons for this. |
| 3. | Leaders had not ensured that all prisoners had sufficient access to their allocated activities. They were taking too long to rectify the issues of low attendance across employment, skills and work. |
| 4. | Leaders had not increased the number of full-time spaces in education. |
| 5. | Leaders had not implemented an effective reading strategy to develop prisoners’ reading further. |
| 6. | Leaders had not ensured that all prisoners had access to a curriculum that supported their wider development. |
| Key concerns | |
| 7. | There was no ‘whole-prison approach’ to supporting the most challenging and vulnerable prisoners, especially those who were self-isolating. Many wing staff told us they did not have a role in the support plans for these individuals. |
| 8. | Too many cells were small and cramped, particularly when two prisoners were sharing. |
| 9. | Although funding for remedial work on E wing had been approved, no start date had been set. This meant that many prisoners continued to live in poor conditions. |
| 10. | Leaders did not have an accurate oversight of the progress that prisoners made towards their learning goals and skills development in industries and work. |
| 11. | Too often, visits started late, which was a source of frustration for prisoners and their visitors. |
| 12. | Key work remained disappointing and did not support progression. Too few sessions were taking place. |
Notable positive practice (Back to top)
We define notable positive practice as evidence of our expectations being met to deliver particularly good outcomes for prisoners, and/or particularly original or creative approaches to problem solving. Inspectors found seven examples of notable positive practice during this inspection, which other prisons may be able to learn from or replicate.
| 1. | Patients had good access to diagnostic equipment, such as bladder scanning and respiratory function testing. This improved the quality of assessments and supported timely referrals to secondary care (see Primary care and inpatient services). |
| 2. | The GP visited the most complex patients on the wings, which improved their engagement with health services and ensured they had access to treatment (see Primary care and inpatient services). |
| 3. | The health and well-being champions (HAWCs) provided valuable peer support and were appropriately trained, coordinated, supported and supervised (see Promoting health and well-being). |
| 4. | Leaders, health care staff, prisoners and a university partner co produced resources to support prisoners with autism (see Mental health). |
| 5. | A multidisciplinary safer prescribing committee ensured that decisions on prescription medications were safer and better coordinated. The committee routinely involved prescribers, substance misuse staff and a psychiatrist (see Medicines optimisation and pharmacy services). |
| 6. | A good range of in‑cell workbooks were provided by the Prison Advice and Care Trust (PACT). Detailed notes of learning outcomes were recorded electronically (see Opportunities for prisoners to progress). |
| 7. | There was good attendance at the risk management meetings to discuss the release of high-risk prisoners. Community probation workers and the police attended meetings on prisoners managed under multi-agency public protection arrangements (MAPPA) (see Returning to the community). |
Unless otherwise specified, these examples are not formally evaluated, are a snapshot in time and may not be suitable for other establishments. They show some of the ways our expectations might be met, but are by no means the only way.
Section 1: Leadership (Back to top)
Leaders provide the direction, encouragement and resources to enable good outcomes for prisoners.
The governor had been in post for 12 months, following a period of significant instability after the departure of a long serving predecessor, during which there had been four governors and four deputy governors in charge. She inherited an experienced staff group, with fewer than 8% having less than two years’ service, which made sure day to day operations were carried out competently. However, despite this depth of experience, the prison had not made progress since our last inspection and was failing in its role as a training and resettlement establishment.
Recognising that the prison had not kept pace with wider change in HMPPS, the governor had reset expectations, including on staff professional standards. While necessary, this action, combined with high levels of sickness absence and other resourcing pressures, reduced frontline capacity and put additional strain on operational delivery.
Since the last inspection, the prison had experienced higher levels of self‑harm, three suicides in custody, a further suicide soon after release, and a suspected homicide. Leaders responded appropriately by strengthening case management and reinforcing day‑to‑day responsibility of staff for safety. Leadership in this area was now credible, with early signs of improvement. Leaders also acknowledged the destabilising impact of illicit drugs, particularly psychoactive substances. They had reset their approach by strengthening oversight of the drug strategy and responses to ‘under the influence’ incidents. However, despite these efforts, illicit drugs remained readily available and continued to undermine leaders’ efforts to keep prisoners safe.
The regime had been simplified to improve consistency and accountability. However, this had not delivered sufficient time out of cell or effective oversight of education, skills and work, and attendance remained too low to support progression.
Population change, including higher turnover, shorter stays and more prisoners from out of the area, increased the complexity of resettlement work and put pressure on delivery. Against this backdrop, offender management was a relative strength, with improved leadership to support prison offender managers in delivering key areas of sentence management and progression.
Self assessment identified the right priorities in safety, regime delivery and leadership capability. However, it remained heavily framed around past instability, rather than demonstrating what the current team were doing to improve outcomes now. As a result, ownership of the forward direction and evidence of its effect on daily practice were not yet clear in all areas.
Overall, the governor brought determination, realism and moral authority to a difficult first year, stabilising the prison and resetting priorities.
Section 2: Safety (Back to top)
Prisoners, particularly the most vulnerable, are held safely.
Early days in custody
Expected outcomes: Prisoners transferring to and from the prison are safe and treated decently. On arrival prisoners are safe and treated with respect. Risks are identified and addressed at reception. Prisoners are supported on their first night. Induction is comprehensive.
| HMIP prisoner survey | Yes | Compared with similar prisons |
| On your first night in this prison, was your cell very/quite clean? | 33% | Lower |
| Before you were locked up on your first night here, were you offered a shower? | 22% | Lower |
Reception was a calm environment where prisoners were welcomed and supported by a peer worker.

Transport often arrived late in the day, leaving little time for new arrivals to settle before overnight lock up.
Safety interviews were rushed and lacked sufficient depth to identify vulnerability and immediate risk. Prisoners were encouraged to answer only ‘yes’ or ‘no’ and to wait until seeing a nurse before discussing self harm. Staff also carried out only one welfare check on the first night, which increased risk.
First night cells were not always clean or adequately equipped. Some lacked basic items such as waste bins and cleaning materials, and one new arrival had no light and a broken phone three days after arriving.


Induction was multidisciplinary and new arrivals had good support from peer workers. However, oversight of the process was insufficient, some written materials were out of date, and there was no system for tracking when prisoners had completed all elements of induction.
It could take up to a week for prisoners to be issued with a prison laptop. This led to long queues to use the electronic kiosks for essential tasks, such as choosing menu items, during the limited time out of cell on the induction unit.
Promoting positive behaviour
Expected outcomes: Prisoners live in a safe, well ordered and motivational environment where their positive behaviour is promoted and rewarded. Unacceptable conduct is dealt with in an objective, fair, proportionate and consistent manner.
Encouraging positive behaviour
| Data provided by the prison | |
| Rate of assaults per 1,000 prisoners in the 12 months to January 2026 | 218 |
| Number of prisoner-on-prisoner assaults (including fights) in the 12 months to January 2026 | 121 |
| Number of prisoner-on-staff assaults in the 12 months to January 2026 | 34 |
The prison felt safe and well ordered. The rate of assaults on prisoners and staff was higher than at our last inspection, but was still below the average for similar prisons, with few recorded as serious. However, more than a quarter of prisoners who responded to our survey (27%) said that they currently felt unsafe.
A prisoner’s death in 2025 was being investigated as a suspected homicide.
Leaders encouraged staff to take a less punitive approach to low-level rule-breaking and focus more on rewarding positive behaviour. Nevertheless, prisoners said that staff frequently issued behaviour warnings for trivial matters and hardly ever recognised good work, which was reflected in prison data on electronic case note entries.
Opportunities to motivate prisoners were available, such as trusted peer work roles and progression to Clive House (see Living conditions and Opportunities for prisoners to progress). However, these were not clearly articulated in the safety strategy, or promoted during induction, and were not used as behavioural targets for the most challenging prisoners.
All violent incidents were investigated promptly and to a reasonable standard. Requests from residential staff to open challenge, support and intervention plans (CSIP – see Glossary) for the most risky or vulnerable prisoners had recently increased.
While those subject to CSIP were discussed briefly at the weekly safety intervention meeting, we found little evidence of day-to-day challenge or support for these prisoners on the wings. The prisoners were also identified for ‘priority’ key work sessions (see Staff-prisoner relationships), but these were infrequent and cursory. Several prisoners who were self-isolating, many due to debt and threats associated with the use of illicit drugs, told us they were unlocked for 30 minutes a day for a shower and exercise but had no meaningful interaction with staff.
Managers used data reasonably well to understand the factors undermining safety, and debt was identified as a significant driver of violence. However, work to address this remained under‑developed (see Suicide and self‑harm prevention). Leaders had strengthened CSIP assurance processes, which helped identify effective practice and improve the quality of plans.
In 2025, the number of adjudications had increased by 70% from the previous year. Leaders recognised that this was partly due to an increase in the number of charges relating to the use of illicit drugs. However, they had been too slow to adjust sanctions to address emerging trends in poor behaviour.
Leaders had successfully reduced the backlog of hearings. Recently, most charges laid at Stoke Heath, especially those relating to violence, had been dealt with promptly.
Use of force
| Data provided by the prison | |
| Total use of force incidents in the 12 months prior to the inspection | 281 |
| Number of times batons drawn in the 12 months prior to the inspection | 5 |
| Number of times batons used in the 12 months prior to the inspection | 1 |
| Number of times PAVA used in the 12 months prior to the inspection | 2 |
The number of use of force incidents had been reducing in the 12 months prior to the inspection and was now among the lowest of similar prisons.
Most uses of force were spontaneous and relatively low level. Very few incidents involved staff using pain-inducing techniques. Batons and PAVA were hardly used, and the number of prisoners reporting injuries from force had reduced in each of the previous two years.
Five of the 30 occasions force was used in January were to protect prisoners who were under the influence of illicit drugs. In the previous year the prison had recorded many examples where a prisoner’s consumption of suspected psychoactive substances had resulted in unpredictable and violent behaviour.
Weaknesses in the governance of use of force had recently been addressed, and the use of body worn video cameras had improved. In the footage we reviewed, force was justified and promptly de escalated, with officers giving clear and calm instructions.
Segregation
The average length of stay in segregation was low, at under four days. Several prisoners had been placed in the unit to protect them from harm after repeatedly being found under the influence of drugs (see Security), because it was more difficult to access illicit substances in segregation.
A dedicated supervising officer had been appointed and was beginning to improve systems and culture. We observed polite and helpful interactions between staff and prisoners, and this was reflected in comments from prisoners who had spent longer in the unit. Segregation staff also received reflective practice sessions from the psychology team, which helped them to manage complex behaviour more thoughtfully and consistently (see Opportunities for prisoners to progress).
Living conditions were not good enough. Cells were worn and scruffy and the showers were grubby and smelled of damp.
Leaders had asked residential managers to develop reintegration plans for prisoners reluctant to leave the unit, but the plans we saw were poor and had not yet been effective in supporting prisoners to return to a normal location.
Security
Expected outcomes: Security and good order are maintained through an attention to physical and procedural matters, including effective security intelligence and positive staff-prisoner relationships. Prisoners are safe from exposure to substance misuse and effective drug supply reduction measures are in place.
| HMIP prisoner survey | Yes | Compared with last time |
| In this prison is it easy/very easy to get illicit drugs? | 55% | Higher |
| Data provided by the prison | |
| Percentage of prisoners testing positive following a mandatory drug test in the 12 months to December 2025 | 31% |
Procedural security measures were appropriate to the population. The arrangements for moving prisoners around the prison worked particularly well. However, some aspects of physical security were weak; for example, there was no enhanced gate security in place, and routine searching of staff and visitors was limited. Leaders had sought to mitigate this risk though ad hoc searches and responded promptly where concerns about staff conduct were identified.
Despite these weaknesses at the gate, leaders understood that illicit drugs were one of the most significant threats to stability and had taken a range of measures to limit their impact once drugs entered the prison. Cell searches were usually carried out promptly, and over 50% resulted in finds. In the previous 12 months, the rate of finds of drug equipment was the highest among all category C prisons.
However, drugs, particularly psychoactive substances, remained too readily available. In February 2026, there were over 150 incidents involving prisoners under the influence, with several requiring immediate medical intervention (see Support and treatment for prisoners with addictions and those who misuse substances). The mandatory drug testing rate over the previous year was higher than in similar prisons. The most frequently detected drugs were psychoactive substances, and the rate of positive tests for those alone over the previous six months was the highest of all category C prisons.
Safeguarding
Expected outcomes: The prison provides a safe environment which reduces the risk of self-harm and suicide. Prisoners at risk of self-harm or suicide are identified and given appropriate care and support. All vulnerable adults are identified, protected from harm and neglect and receive effective care and support.
Suicide and self-harm prevention
There had been four self‑inflicted deaths since the last inspection, including one shortly after release. Work to implement Prisons and Probation Ombudsman recommendations had been far too slow to begin, although this was now in progress.
The rate of recorded self-harm had increased since the last inspection and was now among the highest of all category C prisons.
Leaders had developed a sound understanding of the main reasons for self‑harm, including substance misuse, debt and the amount of time prisoners spent locked up. However, there was too little prison‑wide work to address these causes and prevent self‑harm in the first place (see Time out of cell).
Instead, leaders had focused on improving the support provided after incidents, recruiting extra staff to the safety team and improving multidisciplinary case management. This had produced notable improvements for a small number of prisoners with very complex needs, including reductions in the frequency and severity of self-harm incidents and less need for constant supervision.
There were several positive well-being initiatives, including therapy dogs, workbooks on coping skills, mental health gym sessions and peer support. However, support plans did not always draw on the full range of available interventions, which limited their impact.
Access to Listeners (prisoners trained by the Samaritans to provide confidential emotional support to their peers) was good. The prisoners we spoke to said they felt well supported by the Samaritans and that the safer custody team took their feedback seriously.
Protection of adults at risk
There was no up-to-date local safeguarding strategy and no links with the local authority safeguarding board. While healthcare staff had access to Shropshire Community Health NHS Trust safeguarding policies and wider West Midlands guidance, this did not constitute a prison‑level safeguarding strategy or active multi‑agency safeguarding oversight.
Some internal safeguarding investigations had been carried out by the safety team, but these were not always sufficiently detailed. The chaplaincy undertook some good work to counter extremist ideologies and protect prisoners from them (see Faith and religion).
Section 3: Respect (Back to top)
Prisoners are treated with respect for their human dignity.
Staff/prisoner relationships
Expected outcomes: Prisoners are treated with respect by staff throughout their time in custody and are encouraged to take responsibility for their own actions and decisions.
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Do you have a named officer (key worker)? | 56% | Lower |
In our survey, 65% of prisoners said that staff treated them with respect, which was similar to the previous inspection and other category C prisons. We routinely observed friendly and professional interactions between staff and prisoners. However, staff were too often based in offices, leaving landings unsupervised. Prisoners could identify staff they would approach for help, and most comments we received about staff were positive.
Key work delivery was weak, with too few sessions that were inconsistently delivered and often too brief. This limited their value in helping staff build and sustain positive relationships on the wings (see How staff were supporting prisoners and managing risk).
The widespread use of peer mentors was a strength. Well-trained and supervised prisoners provided valuable support services, and those we spoke to felt well supported. Peer roles were also widely recognised as a route for progression.
Daily life
Expected outcomes: Prisoners live in a clean and decent environment and are aware of the rules and routines of the prison. They are provided with essential basic services, are consulted regularly and can apply for additional services and assistance. The complaints and redress processes are efficient and fair.
Living conditions
Too many prisoners lived in shared cells that had been designed for single occupancy. These did not have enough space, storage or furniture, or lockable cabinets for personal items. There was no privacy when using the toilet. By contrast, standard single cells and the dormitory accommodation on D wing were reasonably well equipped, and prisoners generally had good access to clothing, cleaning materials and showers. Clive House, the small category D unit outside the main prison, offered much better equipped and more spacious accommodation for those assessed as suitable for less restrictive conditions.
Prisoners and staff consistently raised concerns about damp and mould, particularly on E wing. Leaders told us that funding had been allocated for roof repairs and electrical works to fix non‑functioning sockets, but work had not yet begun.
Communal areas, both internal and external, were generally clean and tidy, although some showers were grubby. Wing painters maintained the landings and cells to a good decorative standard, and effective measures were in place to manage vermin.

Residential services
The relatively small kitchen was clean and well-maintained, and operated effectively. Catering staff and prisoner workers collaborated well to produce a varied menu that met the needs of the population.
Serveries across the prison were reasonably clean; however, some food trolleys were in an appalling state. On some wings, staff did not manage the hotplates effectively to ensure that prisoners used appropriate protective clothing, followed safe food service practices and received fair portions.

Prison shop orders were submitted through in‑cell technology, with weekly deliveries available to all men. Newly arrived prisoners could wait up to two weeks for their first full order. However, this was partly mitigated by an improved reception pack and the likelihood that prisoners would arrive with items from previous establishments.
There were no hard copy catalogues, which created further barriers, particularly when ordering items such as stereos, clothing and footwear. Prisoners often relied on family members or staff to identify product codes or order details, which made accessing basic goods unnecessarily difficult.
Prisoner consultation, applications and redress
Consultation arrangements were reasonable. Wing forums operated effectively, and issues raised by prisoners were escalated to the prisoner council. However, the inconsistent frequency of the main consultation meeting undermined prisoners’ confidence in the process.
Complaint forms were easy for prisoners to access and the process was generally well managed. Quality assurance was effective. Property was the most common subject of complaints, accounting for around a quarter of all submissions. This required urgent attention from managers.
Most applications were submitted electronically, and prisoners told us they were usually answered fairly and within expected timescales.
Provision for legal visits was adequate, and capacity met demand. However, these visits took place in the main visits hall, which was not always sufficiently private for confidential discussions. A video‑court facility was available for remote legal interviews, and prisoners had access to relevant prison policies and a useful range of legal textbooks in the library.
Fair treatment and inclusion
Expected outcomes: There is a clear approach to promoting equality of opportunity, eliminating unlawful discrimination and fostering good relationships. The distinct needs of prisoners with particular protected characteristics (see Glossary) or those who may be at risk of discrimination or unequal treatment, are recognised and addressed. Prisoners are able to practise their religion. The chaplaincy plays a full part in prison life and contributes to prisoners’ overall care, support and rehabilitation.
In our survey, prisoners with certain protected characteristics, particularly young, minority ethnic and Muslim prisoners, reported more negative experiences in key areas of daily life than those from other groups.
Prisoners that we spoke to on some wings reported disrespectful treatment and insensitive language from a small number of officers. Leaders were aware of these issues and had dealt robustly with inappropriate behaviour.
Managers had also undertaken a training course called ‘In Their Shoes’ to improve their understanding of different groups, and there were plans to run a similar course for officers. Staff were also encouraged to take a Makaton course to improve communication.
Use of equality data had improved since the last inspection. However, this had not been used strategically by senior leaders to explore or address longstanding disproportionate outcomes for some groups, including Muslim, neurodivergent and younger prisoners, at a whole prison level.
Consultation remained underdeveloped. Forums for specific groups were held up to four times a year; some were very good, but most were poorly attended and did not focus sufficiently on understanding the prisoners’ needs and experiences. This limited leaders’ ability to target improvement.
Disabled and neurodivergent prisoners were generally well supported. Reasonable adjustments and adaptations were made promptly, and a range of interventions helped neurodivergent prisoners to build coping skills in custody and after release. Wing staff were usually aware of prisoners’ needs, although written evacuation plans for those requiring assistance lacked detail.
Support for care leavers was reasonably good. They were helped to access the local authority services that they were entitled to, and an external charity held social coffee mornings for them. However, in our survey, care leavers were more likely than other prisoners to report bullying and to have developed a drug or alcohol problem in prison.
Complaints about discrimination were generally investigated well, and it was positive that recommendations to improve practice were made even when a complaint was not upheld.
Faith and religion
Faith provision remained good. Despite longstanding vacancies in the chaplaincy team, prisoners from smaller faith groups were given opportunities to meet at least fortnightly.
There were good links with community faith groups, who supported prisoners both in custody and after release, despite the prison’s remote location. The chaplaincy team also continued to produce materials and deliver courses aimed at countering extremist ideologies.
Health, well-being and social care
Expected outcomes: Patients are cared for by services that assess and meet their health, social care and substance use needs and promote continuity of care on release. The standard of provision is similar to that which patients could expect to receive elsewhere in the community.
The inspection of health services was jointly undertaken by the Care Quality Commission (CQC) and HM Inspectorate of Prisons under a memorandum of understanding agreement between the agencies. The CQC found there were no breaches of the relevant regulations.
Strategy, clinical governance and partnerships
The head of health care had been absent for four months, which left a gap in strategic direction and oversight.
Clinical leads had taken on some managerial roles, which distracted them from their day-to-day responsibilities. Despite this, the service had maintained good partnership working between health care and the prison.
The risk register was not sufficiently detailed or kept up to date, which undermined clinical governance and scrutiny. Lessons learned from incidents (including safeguarding incidents) and serious investigations were shared. Any changes in practice that had been identified were implemented.
The health care centre did not have enough rooms for service provision. This was particularly notable in secondary mental health care, where the clinical, therapeutic and office spaces were inadequate and inappropriate.
Patients were complimentary about services and gave us examples of good-quality care.
There were few vacancies across the health service, and most gaps were covered by temporary staff, which ensured that services could be provided in key areas of delivery. Clinical supervision was in place and mandatory training for staff was up to date. There were further opportunities for staff development, which contributed to safer patient care.
A recent infection control audit had identified issues that needed to be addressed. These included a failure to replace sinks that did not meet the required standard and to repair flooring in the dental suite.
Feedback was gathered from patients and used to inform service development.
The health care complaints process was not well advertised. The number of complaints was low and responses were dealt with in a timely manner.
Emergency medicines and equipment were located around the prison and checked daily.
Promoting health and well-being
There was no prison‑led health and well-being strategy to coordinate health promotion activities.
The health and well-being champions (HAWCs) identified at the previous inspection continued to provide valuable peer support. These prisoners had developed an impressive skillset and were active in the prison in supporting well-being. They were available as a resource and to signpost prisoners to other services, but also undertook simple procedures, such as weight and blood pressure monitoring. They were all well coordinated, trained and supervised.
A range of health promotion materials were available to provide information and encourage self-care. These included posters, leaflets, laptop‑based information and podcasts. Screening programmes and vaccinations were offered to all patients.
Patients had good access to sexual health services, and there were clear pathways for onward referral.
Disease outbreak plans were in place. During the inspection, we observed the prison managing an outbreak of TB, including contact tracing and testing. This was effective in minimising cross‑infection risks.
Primary care and inpatient services
Patients had access to a good range of primary care services.
Appointments were available all week. The waiting time for a routine GP appointment was 12 days, and emergency slots were available daily. It was notable that the GP visited the most complex patients on the wing, which improved patients’ engagement and ensured they received better care.
All new patients were assessed in reception, including those who arrived late. Most secondary screening was undertaken within seven days.
Patients with long-term conditions were managed well and received a personalised care plan. Clinicians could use diagnostic tools, including bladder scanning and respiratory nitric oxide tester. This had improved assessment times and access to targeted treatment.
Hospital escort capacity was insufficient for the population. However, cancellations and rearranged appointments were well managed.
In a three-month period (December 2025 to February 2026) emergency responses for patients suspected to be under the influence of illicit substances averaged 9.5 per day and placed a significant demand on services. However, patient care was consistently maintained at the appropriate standard.
All planned releases were reviewed, and prisoners were provided with information about accessing NHS and community health services on release, alongside condoms and any medication to take home.
Social care
There was a comprehensive memorandum of understanding between the prison and the local authority. In the last six months, seven prisoners had been assessed for social care, but none required a care package and there had been no social care packages in place for over a year. Prisoners whose referrals were pending assessment received appropriate ongoing care while they waited.
Equipment and adaptations were supplied directly by Shropshire Community NHS Trust (ShropCom), enabling timely delivery and installation for prisoners who required additional mobility aids.
Mental health
Since the previous inspection, ShropCom had subcontracted Midlands Partnership NHS Foundation Trust (MPFT) to provide secondary care while retaining responsibility for delivering primary care. Staff shortages across both teams had impacted on services. Although most posts had been recruited to, leaders recognised that more needed to be done to strengthen joint working. The primary mental health lead had limited capacity, as they were also covering senior management duties. This hindered progress.
Patients’ mental health needs were identified on arrival, and demand for services remained high. ShropCom acted as the single referral point, receiving an average of 103 referrals each month. Agreed referral processes had been reinforced to support daily clinical triage.
The mental health service relied on agency nurses. While this provided consistency, the service did not always manage to operate seven days a week. The specialist counsellor service had only recently resumed after a gap of a year. Although ShropCom offered an appropriate range of primary interventions, delivery was restricted by staffing levels and skills. Resources for prisoners with autism had been developed in partnership with the prison, prisoners and Derby University. These included a range of self-help booklets and information guides that supported prisoners to explain their needs and how staff could best support them.
Governance of MPFT services was strong and the team included an appropriate mix of health professionals, including psychologists. At the time of the inspection, 78 patients with severe and enduring mental health needs were on the caseload. The Care Programme Approach (CPA) framework was followed, clinical records were of good quality and access to psychiatry was good. Pre release arrangements supported continuity of care, including timely liaison with community mental health services.
Seven patients had required hospital transfer under the Mental Health Act in the previous year; the longest wait had been 45 days. No mental health awareness training has been delivered to prison staff.
Support and treatment for prisoners with addictions and those who misuse substances
All new prisoners were offered support on arrival and during induction. A range of psychosocial and clinical substance misuse treatments were available following referral and delivered across the prison.
Clinical notes and care plans were person-centred and met national standards. Patients told us they felt involved in decisions about their care.
The clinical team supported 100 patients on opiate substitution therapy and an additional 23 on long-acting buprenorphine (LAB). There had been good uptake and outcomes in the use of LAB.
Patients had access to groups facilitated by the psychosocial team and excellent support from the HAWCs (see Promoting health and well-being).
Unfortunately, services such as Alcoholics Anonymous and Narcotics Anonymous were not available.
Every patient found using illicit drugs or alcohol was seen by staff for a harm reduction intervention.
In February 2026 there were 156 cases of patients suspected to be under the influence of illicit substances. This had a significant impact on Forward Trust’s ability to maintain service delivery.
An incentivised substance-free living wing and recovery wing were available, but neither provided sufficient support for those with long-term addiction issues. Psychosocial services attended the wing when a patient was suspected to be under the influence or in crisis, or to deliver an ongoing course.
The service provided strong continuity of care when patients returned to the community. Staff made timely referrals to community services and arranged prescriptions ahead of release. Patients were provided with harm reduction information, training and a supply of naloxone to help keep them safe.
Medicines optimisation and pharmacy services
There was suitable access to a wide range of medicines, which were dispensed in a safe and timely fashion. Administration was carried out safely, and missed doses were followed up by members of the team. However, supervision by officers was inconsistent, which could provide opportunities to conceal medicines.
There were regular medicine management meetings, but these did not routinely involve a prescriber. This reduced the strategic ability to further improve the service or identify trends. There were gaps in the in-possession risk assessment process, which meant patients were not always reviewed within designated timescales.
Clinical screening was carried out by a pharmacist. However, the lack of structured pharmacy services was a missed opportunity to advise patients directly.
Tradeable medicines were monitored, with some audits undertaken. But work to ensure these medicines were suitably optimised could be improved.
A safer prescribing committee helped with making important decisions about prescriptions to ensure the correct care was provided. The committee was multidisciplinary, and routinely included prescribers from the primary care team, substance misuse services, and a psychiatrist. It provided diverse and specialised clinical perspectives, which helped to ensure more accurate decisions, safer care, and better coordinated treatment plans for each patient, and to improve patient outcomes.
Dental services and oral health
A permanent dental team was on site three days per week to triage, assess and treat patients. At the time of the inspection, 165 patients were waiting for a routine appointment, with an average wait of five weeks. These waiting times were reducing following the addition of an extra dentist.
Governance of the service was strong, with regular auditing of key processes. Staff were up to date with essential training and felt well supported.
Equipment was well maintained, and infection control was good. However, flooring around the dental chair was now a risk and required replacing. This issue had been reported to the prison over three months ago and was yet to be actioned, which was unacceptable.
Section 4: Purposeful activity (Back to top)
Prisoners are able and expected to engage in activity that is likely to benefit them.
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Do you usually spend less than two hours out of your cell each day on Mondays – Fridays? | 49% | Higher |
| Do you usually spend less than two hours out of your cell each day on Saturdays – Sundays? | 73% | Higher |
| In a normal week can you get association three times or more? | 87% | Higher |
| HMIP time out of cell data (at the time of the inspection) | |
| Average proportion of prisoners locked up during the working day | 25% |
Time out of cell
Expected outcomes: All prisoners have sufficient time out of cell (see Glossary) and are encouraged to engage in recreational and social activities which support their well-being and promote effective rehabilitation.
The current regime had increased participation in activity during the working day, and the proportion of unemployed prisoners had reduced to around 12%. However, although all work and training places were allocated, attendance was too low and many activity sessions ran below capacity, which limited the regime’s overall effectiveness. Prisoners could sometimes choose between going to work and remaining on the wing for association, showers or exercise, and too many prisoners in this training prison still spent the core day locked in their cells.
Access to PE facilities was good. Both gyms were well attended, and staff made appropriate efforts to balance work attendance with opportunities for recreational gym use. Prisoners benefited from positive initiatives such as a weekly parkrun, and the prison was due to receive significant upgrades to PE equipment shortly after the inspection. However, the lack of usable outdoor sports pitches and the absence of accredited PE qualifications continued to limit the range of activities available and their value for prisoners’ progression.



The pleasant and well‑stocked library provided an excellent environment for prisoners to develop an interest in reading. The lead librarian had a notably positive impact, and worked closely with staff to ensure equitable access for prisoners across the establishment. However, the prison’s reading strategy was weak, and we found little evidence that it had any meaningful influence on the wider life of the prison or on prisoners who were less confident readers.
Education, skills and work activities
Ofsted inspects the provision of education, skills and work in custodial establishments in England. The following summary has been provided by Ofsted inspectors who attended this inspection. Their full report is published under ‘Further resources’.
Ofsted made the following assessments about the education, skills and work provision:
- Overall effectiveness: Inadequate
- Quality of education: Requires improvement
- Behaviour and attitudes: Requires improvement
- Personal development: Requires improvement
- Leadership and management: Inadequate
Leaders had not fully rectified most of the weaknesses found at the previous inspection. They had not ensured that all prisoners could access sufficiently their allocated activities. The structure of the regime meant that prisoners could not attend all education, skills and work sessions due to clashes with other activities, such as association. This meant that attendance was not high enough. Leaders had not increased the number of full-time places, which meant prisoners took longer to complete their qualifications.
Leaders mostly had an effective oversight of the quality of the education, skills and work provision. The quality of training prisoners received had improved. However, there was a lack of sufficient challenge and oversight from senior leaders. In a very few instances, improvements had been too slow.
Leaders did not have an effective whole prison reading strategy that promoted reading across the prison estate.
Achievement rates varied too widely across courses due to prisoners leaving their programme early because of transfer. However, most prisoners that remained on their qualifications achieved them.
Allocations were fair and timely and mostly met prisoners’ needs. However, in a very few instances, prisoners’ allocations did not fully align with their intended next steps and wing work fell out of the main allocation process.
The pay for prisoners was fair and equitable, with education rates aligned to other roles and higher pay used appropriately to recognise trusted roles such as mentors.
Leaders had developed education and skills curriculums that mostly met the needs of prisoners and local and regional skills shortages. They had engaged with a range of employers to provide courses that developed the skills prisoners needed to gain employment upon release.
Prisoners who had learning difficulties and/or disabilities received effective and targeted support. Teachers and instructors planned their lessons and work to meet prisoners’ individual needs effectively. Prisoners with additional needs achieved as well as their peers.
Teachers mostly taught topics in a well-considered sequence. They mostly used effective teaching strategies. However, in a few instances the pace of sessions was too slow. Teachers did not provide prisoners with the explanations needed to move on to their next task. This meant that they did not develop their knowledge as quickly as they could.
Instructors did not have an accurate oversight of the progress that prisoners made towards their learning goals and skill development. In industries, prisoners did not always make the progress of which they were capable.
Prisoners in education benefited from discussions on a range of topics that helped to develop their self-awareness and improve their confidence. However, prisoners in industries and work did not access a curriculum that supported their wider development.
On arrival, prisoners received effective information, advice and guidance that helped them to make informed choices about their short- and longer-term goals linked to their transfer or release.
Prisoners due for release were prepared well for employment. They received individual support on topics such as disclosure, how to create a CV and searching for employment.
Section 5: Preparation for release (Back to top)
Preparation for release is understood as a core function of the prison. Prisoners are supported to maintain and develop relationships with their family and friends. Prisoners are helped to reduce their likelihood of reoffending and their risk of harm is managed effectively. Prisoners are prepared for their release back into the community.
Children and families and contact with the outside world
Expected outcomes: The prison understands the importance of family ties to resettlement and reducing the risk of reoffending. The prison promotes and supports prisoners’ contact with their families and friends. Programmes aimed at developing parenting and relationship skills are facilitated by the prison. Prisoners not receiving visits are supported in other ways to establish or maintain family support.
The prison’s rural location meant that many prisoners were held far from home. Recent data suggested that 352 men had not received a visit in the previous 12 months.
In-cell telephones, the email-a-prisoner scheme and secure video calls provided other forms of contact; however, on weekdays, video calls were only available in the mornings, which meant that prisoners could not speak to their children after school.
Face‑to‑face visits were limited to afternoons on Tuesday to Thursday and at weekends. Visits often started late, which was a big source of frustration for prisoners and their families.
The visits hall was well presented, and it was encouraging to see a varied range of refreshments, including several hot options.



The PACT provided the family services. Provision was good: visitors were warmly welcomed and creative initiatives such as the ‘Worry Monster’ and ‘William the Bear’ helped to support children.


Efforts to gather family feedback through forums had led to useful discussions, although attendance remained low.
Monthly family days were well attended; they offered families valuable time together, with a range of games. However, they did not run for the full day, and some prisoners were unclear about the criteria for attendance. An equivalent session was held every quarter for those who did not receive any visits.
Escorts for prisoners to visit dying or seriously ill relatives were well managed.
Reducing reoffending
Expected outcomes: Prisoners are helped to change behaviours that contribute to offending. Staff help prisoners to demonstrate their progress.
How staff were supporting prisoners and managing risk
The offender management unit (OMU) leadership team was well established and effective. Caseloads were in the mid‑fifties which, combined with high turnover and the fact that two‑thirds of prisoners posed a high or very high risk of serious harm, made the work challenging.
Prison offender managers (POMs) generally felt well supported and received regular supervision from managers, which they valued. They worked within pod structures made up of prison and probation staff, and demonstrated good knowledge of the individuals they managed.
Prisoners we spoke to could name their POMs and generally reported good relationships. The centrally located OMU was accessible by appointment using movement slips, and two trained peer workers maintained effective links with the wings.
Early contact was usually good, supported by clear initial tasks, but later engagement often became reactive. While many POMs carried out proactive work to support prisoners and manage risk, in a small number of cases ongoing contact was weak.
This was similar to the position at the last inspection, although the balance was now more positive. Prisoners we spoke to, including those serving indeterminate sentences, were particularly complimentary about the support they received from their POMs.
In one impressive example, a POM delivered 11 structured one‑to‑one sessions, each lasting 80 minutes, informed by input from a psychologist and focused on childhood experiences. The prisoner said this had helped him to understand his previous violent behaviour.
Prisoners made good use of in‑cell laptops to contact their POMs. These exchanges were often recorded electronically, which gave prisoners a clear voice in the case notes. However, in a few cases this appeared to replace face‑to‑face contact.
Key work did little to support progression. Although some electronic case note entries were of decent quality, the limited frequency and reach of sessions meant these did not contribute effectively to wider rehabilitative goals (see Staff-prisoner relationships).
OASys assessments were of good quality and completed by POMs. Processes dependent on up‑to‑date assessments were not delayed, and governance was strong. Work on recategorisation and home detention curfew was also of good quality, and delays were typically outside the prison’s control.
Specific groups received appropriate attention. For example, younger prisoners were often allocated to POMs with relevant experience, and while prisoners serving indeterminate sentences for public protection (IPP) received limited additional support, their progression panels were good, with effective joint working between psychology and the OMU.
Public protection work was better coordinated than at the previous inspection. It was led by an experienced OMU manager who had secured good buy‑in from other departments.
Opportunities for prisoners to progress
The Building Choices programme had begun, replacing previous accredited programmes, and prisoner data indicated a need for all four strands. This represented an improvement on earlier provision, as prisoners with a history of violence or domestic abuse could now access interventions that had previously been unavailable.
Although prisoners were allocated to programmes according to national prioritisation guidelines, many were allocated late in their sentence or shortly before their parole hearing. This left insufficient time to complete courses, particularly for those seeking progression to open conditions.
The psychology team was well embedded and worked collaboratively across departments, attending key meetings and offering a strong consultancy function. Their work included oversight of prisoners serving IPP sentences. They also provided fortnightly reflective practice sessions for segregation staff (see Segregation).
A range of additional interventions were available. These included the Forward Trust’s two‑week Relationships Matter course, which was completed by 21 prisoners in the past year, and PACT’s Coming Home and Within My Reach courses, which were completed by 21 and 16 prisoners respectively. The chaplaincy also continued to run its Living with Loss groups, with 23 prisoners completing the programme.
This was complemented by a good range of in‑cell workbooks provided by PACT. These were marked and learning outcomes were recorded electronically, enabling effective information‑sharing across departments.
Clive House provided a clear progression pathway for suitable prisoners. The small category D facility could accommodate eight men in a self‑contained unit outside the main prison. At the time of the inspection it held five prisoners, who were working in the local community and maintaining family contact through overnight visits.
Returning to the community
Expected outcomes: Prisoners’ specific reintegration needs are met through good multi-agency working to maximise the likelihood of successful resettlement on release.
On average, around 75 prisoners were released each month, an increase since the last inspection and reflecting changes in the prison’s population.
Risk management meetings for high risk prisoners were held monthly and attended by an appropriate range of partners. For prisoners subject to MAPPA (see Glossary) conditions, meetings were appropriately attended by community probation staff and the police. Written contributions were of good quality, and attendance at MAPPA meetings was appropriate.
Support to prepare prisoners for release was very good. During their final three months, the Department for Work and Pensions (DWP) delivered weekly group sessions focused on employability and wider resettlement plans. Prisoners spoke highly of this support, and we observed DWP staff going above and beyond to prepare individuals for release.
The pre‑release team (PRT) met one‑to‑one with low- and medium‑risk prisoners being released to the West Midlands around 12 weeks before release. They explained their rights and the practical arrangements for release. Support for prisoners being released out of the area relied on community probation services.
An increase in out‑of‑area releases had made it more difficult to secure suitable accommodation for all prisoners. Around 40% of those released into the community had sustainable accommodation in place, while 8% were released homeless.
Section 6: About HMP & YOI Stoke Heath (Back to top)
Category of the prison
Closed category C prison for adult males, with a small category D unit outside the main site.
Brief history
HMP & YOI Stoke Heath was built in 1964 as a category C adult prison. Since July 2011 it has held both adults and young adults. In November 2014, it began reconfiguration as a designated resettlement prison for Wales. The resettlement function was reviewed in 2017 and the prison now serves the West Midlands and North West as a category C resettlement and training prison.
Population
At the time of the inspection, Stoke Heath held 741 prisoners. There was operational capacity for 782.
- 1,335 new prisoners were received each year (around 111 per month).
- 6% of the population were foreign national prisoners.
- 30% of prisoners were from black and minority ethnic backgrounds.
- An average of 77 prisoners had been released each month in the 12 months prior to the inspection.
- 318 prisoners were receiving support for substance misuse.
- 100 prisoners were referred for mental health assessment each month, on average.
Short description of residential units
A–E wings – general population
F wing – designated drug treatment unit
G wing – induction and prisoners sentenced to longer terms
I wing – progression and incentivised substance-free living unit
Clive House – open unit holding up to eight category D prisoners
Segregation unit
Prison status (public/private)
Public
Key providers
Physical health provider: Shropshire Community NHS Trust
Mental health provider: Shropshire Community NHS Trust (primary), Midlands Partnership NHS Foundation Trust (secondary)
Substance misuse treatment provider: Midlands Partnership NHS Foundation Trust (clinical), Forward Trust (non-clinical)
Dental health provider: Time for Teeth
Prison education framework provider: Novus
Escort contractor: GeoAmey
Prison group director
Mark Greenhaf, West Midlands
Name of governor and date in post
Rachel James, March 2025
Changes of governor since the last inspection
Jacqui Lane (acting), January 2025 – March 2025
Mark Greenhaf, June 2023 – December 2024
John Huntington, August 2009 – June 2023
Date of last inspection
9 – 23 January 2023
Progress on concerns from the last inspection (Back to top)
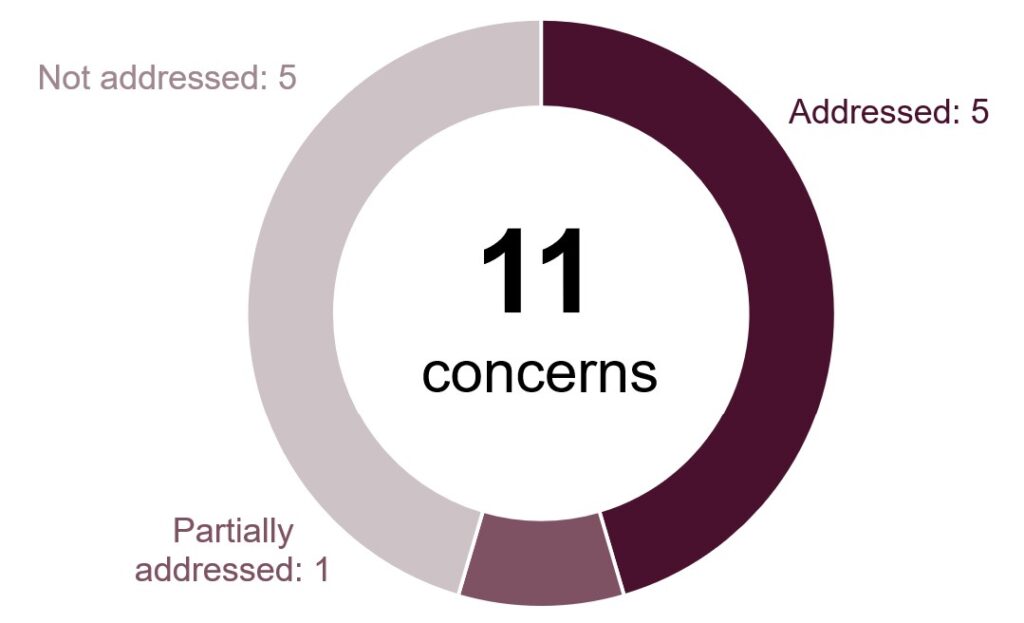
At our last inspection in 2023 we raised 11 concerns, six of which were about areas of priority concern.
At this inspection we found the following progress:
The following is a list of all the concerns raised, organised under the four tests of a healthy prison.
Respect
Priority concern
There was very little key work being delivered. In December 2022 only 5% of sessions had been delivered and entries in case notes showed little evidence of a focus on sentence plan targets.
Not addressed
Key concerns
Too many cells were small and cramped, particularly when two prisoners were sharing.
Not addressed
Consultation with prisoners from protected groups was very limited and the analysis of data was insufficient to identify disproportionate outcomes.
Addressed
Prisoners waited far too long for dental treatment.
Addressed
Purposeful activity
Priority concerns
Prisoners, particularly the unemployed, had far too little time out of cell.
Not addressed
Prisoners’ access to purposeful activity was poor as there were too few full-time places. Attendance and punctuality were not good enough and sessions were often cancelled.
Not addressed
Leaders and managers had not implemented a curriculum that met the needs of all the prison population. There were too few education English and mathematics places and prisoners in work and workshops were not receiving the help they needed to improve their English and mathematics skills or study for relevant qualifications. An effective reading strategy had yet to be implemented.
Partially addressed
Preparation for release
Priority concerns
There were not enough places on accredited programmes to help prisoners address their offending behaviour.
Not addressed
Decisions to grant release on temporary licence were not always sufficiently robust or in line with national procedures.
Addressed
Key concerns
There was not enough support to help prisoners maintain relationships with their families and friends.
Addressed
The application of public protection arrangements was weak.
Addressed
More about this report (Back to top)
This report outlines the priority and key concerns from the inspection and our judgements against the four healthy prison tests. Each of the following four sections contains a detailed account of our findings against our Expectations for men’s prisons.
Find out more about our Expectations and how we inspect
Find out more about priority and key concerns
Find out about notable positive practice
Findings from the survey of prisoners and a detailed description of the survey methodology are published alongside this report. Please note that we only refer to comparisons with other comparable establishments or previous inspections when these are statistically significant. The significance level is set at 0.01, which means that there is only a 1% chance that the difference in results is due to chance.
The tables in this report which provide data from HMI Prisons prisoner surveys also include comparisons with similar prisons.
| Description | What it means |
| Lower | the prison’s percentage is statistically significantly lower than the comparator: prisons with the same function type, or at the last inspection |
| Higher | the prison’s percentage is statistically significantly higher than the comparator: prisons with the same function type, or at the last inspection |
| No difference | the prison’s percentage is not statistically significantly different to the comparator: prisons with the same function type, or at the last inspection |
Inspection team
This inspection was carried out by:
Charlie Taylor, Chief inspector
Ian Dickens, Team leader
Martyn Griffiths, Inspector
Lindsay Jones, Inspector
David Owens, Inspector
Paul Rowlands, Inspector
Nadia Syed, Inspector
Tareek Deacon, Researcher
Phoebe Dobson, Researcher
Alicia Grassom, Researcher
Joe Simmonds, Researcher
Sarah Goodwin, Lead health and social care inspector
Simon Newman, Health and social care inspector
Mark Griffiths, Care Quality Commission inspector
Craig Whitelock-Wainwright, General Pharmaceutical Council inspector
Alison Humphreys, Lead Ofsted inspector
Zoe Ibbotson, Ofsted inspector
Joanne Stork, Ofsted inspector
Find out more about the terms and abbreviations used in this report in our glossary.
Easy read summary and press notice (Back to top)
Survey material and Ofsted full report (Back to top)
The following files may not be suitable for users of assistive technology.
Request an accessible format
If you use assistive technology (such as a screen reader) and need a version of any of these documents in a more accessible format, please email media@hmiprisons.gov.uk. Please tell us what format you need. It will help us if you say what assistive technology you use.