
HMP & YOI Downview
Report on an unannounced inspection of HMP & YOI Downview by HM Chief Inspector of Prisons, 2-12 February 2026

Introduction (Back to top)
Downview, a complex prison located to the south of London, held 302 women at the time of inspection, most of whom were serving sentences longer than four years.
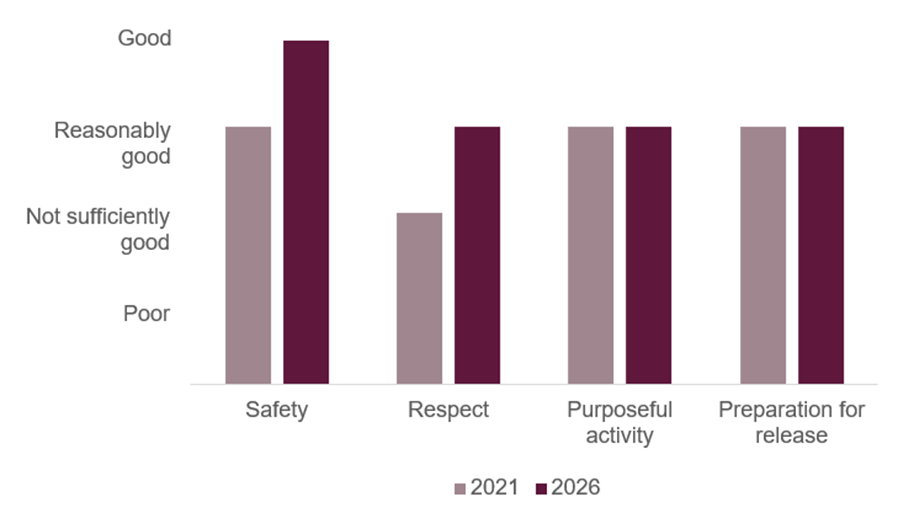
Under the leadership of an experienced governor, our healthy prison assessments improved from reasonably good to good for safety and not sufficiently good to reasonably good for respect. Overall, Downview was a safe, decent, well-run prison in which most women had opportunities to get out of their cells and get into meaningful purposeful activity. There was, however, not enough for women to do on Fridays or at the weekend, so many were locked in their cells for long periods of time.
Relationships between prisoners and staff were generally excellent, but as at our last inspection, the prison was let down by some officers who were rude or dismissive to the women in their care. The governor was beginning to deal with some of these residual staffing issues and was aware of her less well performing staff members. There was a lack of meaningful incentives to support women to behave well which was a missed opportunity to support prisoners’ progression and prepare them to cope on release.
Staff shortages in the offender management unit (OMU) meant women often did not receive regular support, which caused delays in completing statutory tasks such as recategorisation reviews. Although there were some creative interventions, too many women could spend months without talking to anyone about their progress through their sentence. There was also insufficient support for women due to be released with far too many leaving the jail homeless or without sustainable accommodation. Shortages in probation staffing both inside and outside the jail meant some high-risk and vulnerable women did not have their post-release living arrangements confirmed until much too late. In a couple of cases we reviewed, the offer of a place in an approved probation hostel was withdrawn very near to the release date which impacted negatively on effective risk management.
The government’s failure to respond to the April 2025 Supreme Court ruling left prison leaders in a difficult position, creating ongoing uncertainty about the future of the E wing unit for transgender prisoners. Risk assessments to determine the day-to-day management arrangements for each prisoner were robust, including setting out the controls to be applied to limit interactions with the main population,
Many of the women at Downview had addiction issues and had been housed on the incentivised substance free living (ISFL) unit. It was disappointing to see that a proportion continued to take opiate substitution therapy, which undermined the purpose of the unit.
Health inspectors were concerned by the oversight of women with long-term conditions and by the huge delays in getting very unwell women transferred to secure hospital for treatment for serious mental health difficulties.
This was a positive inspection of a jail that had improved since our last inspection. With the continued committed leadership from this governor, inspectors left with some optimism that if the staffing situation can be resolved, the jail will continue to make sustained progress.
Charlie Taylor, HM Chief Inspector of Prisons, February 2026
Outcomes for prisoners (Back to top)
We assess outcomes for prisoners against four healthy prison tests: safety, respect, purposeful activity, and preparation for release (see More about this report for more information about the tests). We also include a commentary on leadership in the prison (see Section 1).
At this inspection of [insert prison name], we found that outcomes for prisoners were:
- Good for safety
- Reasonably good for respect
- Reasonably good for purposeful activity
- Reasonably good for preparation for release.
We last inspected HMP & YOI Downview in 2021. Figure 1 shows how outcomes for prisoners have changed since the last inspection.
Figure 1: HMP & YOI Downview healthy prison outcomes 2021 and 2026
What needs to improve (Back to top)
During this inspection we identified 10 key concerns, of which five should be treated as priorities. Priority concerns are those that are most important to improving outcomes for prisoners. They require immediate attention by leaders and managers.
| Priority concerns | |
| 1. | Some officers were abrupt and dismissive in their interactions and perceptions from women about inconsistencies in the application of rules led to feelings of unfair treatment. |
| 2. | Patients needing treatment under the Mental Health Act waited too long to be transferred to hospital. For example, one patient had waited 156 days. |
| 3. | The management of long-term health conditions was unacceptable. This included poor recording, little face-to-face care planning and the lack of a dedicated nurse. |
| 4. | Resettlement and offender management teams had too few staff. This made the delivery of proactive support and practical help difficult. |
| 5. | There was a lack of sustainable accommodation on release. Some places in approved premises for those presenting a high risk of harm to themselves or others were withdrawn at the last minute. |
| 6. | Incentives and rewards to promote good behaviour were limited. |
| Key concerns | |
| 7. | The availability of illicit drugs, including the trading of prescribed medication, posed a risk to the stability of the prison and to women’s health and well-being. |
| 8. | The application system was unreliable. Many simple requests did not get dealt with. |
| 9. | Most women were locked in their cell for too long on a Friday and over the weekend. |
| 10. | Women working on wings and in industries were not provided with meaningful targets relevant to their work or to help them progress. |
Notable positive practice (Back to top)
We define notable positive practice as evidence of our expectations being met to deliver particularly good outcomes for prisoners, and/or particularly original or creative approaches to problem solving. Inspectors found some examples of notable positive practice during this inspection, which other prisons may be able to learn from or replicate.
| 1. | An on-site shop selling hair and beauty products for black prisoners and those from Asian backgrounds women had been introduced (see Living conditions). |
| 2. | Offender management unit (OMU; see Glossary) staff prebooked the passenger assist service to support the most vulnerable women on release who had to travel long distances by train (see Returning to the community). |
Unless otherwise specified, these examples are not formally evaluated, are a snapshot in time and may not be suitable for other establishments. They show some of the ways our expectations might be met, but are by no means the only way.
Section 1: Leadership (Back to top)
Leaders provide the direction, encouragement and resources to enable good outcomes for prisoners.
| HMIP prisoner survey | Yes | Compared with the last inspection |
| If you want to, can you talk to managers, governors or directors in this prison? | 47% | Higher |
The governor managed two prisons which were 50 miles apart. She had worked hard to improve the jail had a clear and appropriate set of priorities. The leadership team was more visible to prisoners than at our last inspection which was supported by our survey result. Joint working between functions had also improved. The safety team, particularly the skilled middle manager, showed drive and compassionate care and leaders had developed a very effective safety interventions meeting (SIM; see Glossary) to identify, and coordinate individualised support.
Significant leadership drive and focus had improved the quality of key work (see Glossary) which was now more meaningful and supportive of prisoners’ progression. However, leaders had not yet dealt with the attitude of a small number of wing officers who were abrupt and uncaring in their manner. This had led to the perception among some prisoners of unfair treatment.
A new model of resourcing due to start in April 2026 would provide more middle managers on the wings to help address this culture, but these staff members would need considerable support and coaching. The governor had already secured support from an HM Prison and Probation Service (HMPPS) staff training programme called ‘Enable’ and she had commenced the rollout of the ‘Behind the Behaviour’ programme to help staff understand women and their responses to triggers.
The government had failed to issue a revised policy about the management of transgender women since the UK supreme court made its ruling in April 2025 which left many uncertainties for staff and prisoners.
The decision to locate a transgender woman at Downview was made by the HMPPS complex case board and the risk assessment was shared with prison leaders to inform decisions about the day-to-day management, including controlled access to some activities away from the unit.
HMPPS had not prioritised Downview for resources we often see in men’s prisons. There was no enhanced gate security which was a concern given a recent and significant security breach and the prison did not have a body scanner. There was also no in-cell technology to help women deal with their day-to-day lives, such as making applications.
The health care team was well led and provided reasonably good outcomes through strong partnership working. Additional funding from HMPPS and the NHS had allowed leaders to expand the excellent offender personality disorder provision.
In contrast to this, leaders had not adequately resourced offender management or resettlement work and had failed to achieve four out of six concerns from our last inspection.
Leaders engaged with a range of employers to make sure that the education, skills and work curriculum focused on preparing women for employment on release, but they had failed to drive up the use of release on temporary licence (ROTL; see Glossary).
Section 2: Safety (Back to top)
Women, particularly the most vulnerable, are held safely.
Early days in custody
Expected outcomes: Women are safe at all times throughout their transfer and early days in prison. They are treated with respect and well cared for. Individual risks and needs are identified and addressed, including care of any dependants. Women are given additional support on their first night and induction is comprehensive.
Early days arrangements were good. Late arrivals were rare, and prisoners knew their transfer destination. Reception staff treated new arrivals well, for example, they were not locked into the holding room and had access to food and drink.


| HMIP prisoner survey | Yes | Compared with similar prisons |
| Before you were locked up on your first night here, were you offered: support from another prisoner (e.g. Insider (see Glossary) or peer supporters)? | 34% | Lower |
Staff spoke with new arrivals in private and gave helpful information but, although peer workers such as Listeners (see Glossary) were available, they were not easily identifiable and did not offer formal contact with all new prisoners.
Most first night cells were clean and well equipped, and prisoners received a welcome pack with distraction materials and a book, which they appreciated. They could buy telephone credit and basic grocery items, which helped to prevent some from getting into debt. Most had time to settle in, shower and call family or friends before being locked up. Staff also completed additional welfare checks on them during the first night.
Survey respondents were mostly positive about the quality of induction, with 61% saying it covered what they needed to know, which was the same proportion as in the other two training prisons. Although the induction timetable was comprehensive, not all departments delivered their planned session, and peer-led elements lacked staff oversight. Some of the sessions took place in an open and noisy communal area which afforded little privacy. When not engaged in activities, new prisoners spent too long locked in their cells with little to do.
Promoting positive relationships and support within the prison
Expected outcomes: Safe and healthy working relationships within the prison community foster positive behaviour and women are free from violence, bullying and victimisation. Women are safeguarded, are treated with care and respect and are encouraged to develop skills and strengths which aim to enhance their self-belief and well-being.
Safe and healthy relationships
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Do most staff here treat you with respect? | 64% | No difference |
| For those who have a named officer (e.g. key worker or personal officer) is your named officer very/quite helpful? | 75% | No difference |
We saw many attentive and friendly interactions by officers who clearly knew women in their care well. However, as at our last couple of inspections, attitudes and the level of engagement were mixed, and we saw some being abrupt and dismissive with prisoners. Some prisoners said the rules were applied inconsistently which fuelled a perception of favouritism and there were examples of discriminatory comments described to us.
The quality of support received from key workers was excellent. The same officer delivered each session, and there was a good focus on providing practical and emotional support. Some women said they found the sessions beneficial and told us their key worker had resolved important issues for them swiftly. Key workers also played an important role in discussing behaviour and sentence progression with women. However, further improvements were needed to make sure sessions were delivered regularly.
Reducing self-harm and preventing suicide
There had been no self-inflicted deaths since our last inspection. The rate of self-harm was much higher in 2025 than it had been in 2024, but it had begun to reduce in the latter part of the last year. Despite this reduction, the rate remained slightly higher than in the two most similar prisons. A small number of prisoners self-harmed repeatedly, although relatively few incidents were serious. Staff and prisoners described many examples where individuals had been helped to reduce the severity and frequency of their self-harm.
Staff, particularly the safety team, knew prisoners well, and the SIM was effective at putting in place plans for those in need. Women could get support to help them cope better, including psychological services sessions; meaningful key work; access to pleasant outside spaces; and involvement in purposeful activity. Access to Listeners was also good and the two Listener rooms were pleasant.


However, assessment, care in custody and teamwork (ACCT; see Glossary) care plans were often limited and rarely reflected the support available. Inconsistency of case managers frustrated many prisoners, and some of those who were or had been supported by ACCT case management said they had felt uncared for when in crisis.
It was positive that anti-rip clothing had not been used for over two years. Constant supervision was used appropriately and was supportive of the woman in crisis, however, the designated cells were bleak, but staff encouraged prisoners to engage in the regime and return to their own cells at the earliest opportunity.
Protecting women, including those at risk of abuse or neglect
Staff understood the principles of adult safeguarding and prisoners of concern were discussed at the SIM to establish support plans. Links with the local adult safeguarding board had improved.
Promoting positive behaviour
Expected outcomes: Women live in a safe, well-ordered and supportive community where their positive behaviour is promoted and rewarded. Antisocial behaviour is dealt with fairly.
Supporting women’s positive behaviour
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Do you feel unsafe now? | 21% | No difference |
The prison felt safe and calm during our inspection week. Although the rate of violence had increased over the last year it was just below average when compared to the two most similar prisons. Leaders had conducted a thorough analysis of the causes of violence but support for women experiencing bullying or another form of victimisation remained limited. However, the proposed introduction of Peace and Community Engagement (PACE) peer support workers looked promising.
Case management for perpetrators or victims of violence using challenge, support and intervention plans (CSIPs; see Glossary) was applied robustly, but investigations to understand the underlying causes lacked detail.
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Are there opportunities and rewards to motivate people in this prison? | 25% | No difference |
In our survey, few women said they were aware of opportunities and rewards to motivate them to behave well. We found that 80% of the total population were on the highest level of the incentives scheme, with many of these benefiting from more time out of cell, better living conditions and pleasant, well equipped association rooms, including self-catering facilities. The incentives policy was applied consistently, and staff used it effectively including issuing warnings in response to poor behaviour when necessary.

Adjudications
Most charges were appropriate and outcomes proportionate, with 59% found proven. Rehabilitative activities had been introduced, with a focus on referring prisoners who tested positive during mandatory drug testing (MDT; see Glossary) to substance misuse services. There was limited use of payback punishments as an alternative sanction and cellular confinement was used too often.
We saw evidence of neurodiversity support plans being used effectively to understand the reasons behind women’s behaviour.
Segregation
Prisoners spoke positively about their treatment by staff, and we saw examples of excellent support being given to those with complex needs. Subject to a risk assessment, women could serve their period of cellular confinement in their own cells on house units, but governance of these arrangements was poor.
The unit was stark, but the exercise yard had improved since our last inspection with seating, exercise equipment and a mural to brighten up the area. The regime while segregated was limited, with women only getting out of their cell for a shower, exercise and to complete domestic tasks each day. This was of particular concern for those who were acutely mentally unwell and were only in the unit due to the lack of more suitable places within the prison.

Use of force
Force had been used 165 times in the last 12 months which was a higher rate than in the two similar prisons. However, this was reducing and incidents rarely involved full restraint. Over a third of incidents were to prevent self-harm and, of those we reviewed, we found this was not always necessary or proportionate.
The use of body-worn cameras was improving, although some staff did not switch them on early enough to capture the lead up to the incident.
Oversight was strong. Poor practice was challenged and opportunities for learning and upskilling staff were developing. Positively, prisoners were routinely spoken to following any use of force.
Security
Expected outcomes: Security measures are proportionate to risk and are underpinned by positive relationships between staff and women. Effective measures are in place to reduce drug supply and demand.
| HMIP prisoner survey | Yes | Compared with similar prisons |
| In this prison, is it easy/very easy to get illicit drugs? | 39% | Higher |
| In this prison, is it easy/very easy to get medication not prescribed to you? | 45% | No difference |
The installation of additional CCTV had improved coverage across the site, and in response to a notable security incident, improvements had been made to security procedures at the main gate. However, HMPPS had not provided funding to install any technology to enhance this further.
A dedicated residential unit with 16 cells physically separated transgender women from the general population. At the time of this inspection, it held seven prisoners who had been located at the prison following a risk assessment by a multidisciplinary complex case board (CCB) within HMPPS, chaired by a prison group director.
Leaders at Downview could request a review by the CCB of a prisoner’s management should there be a change in risk or individual circumstances. The central team completed checks of case records to maintain oversight of ongoing behaviour and their suitability to remain located on E wing.
The CCB’s risk assessment was supplied to prison leaders to help them assess and determine the day-to-day management arrangements for each prisoner. Management plans set out the controls to be applied to limit interactions with the main population, and the expectations about the level of supervision while on or off the unit were clear. However, we noted that E wing officers would benefit from regular verbal reminders and written information about the restrictions in place for each prisoner.
Section 3: Respect (Back to top)
Women’s relationships with children, family and support networks are central to their care in custody. A positive community ethos is evident, and all needs are met.
Relationships with children, families and other people significant to women
Expected outcomes: Women are able to develop and maintain relationships with people significant to them, including children and other family members. The prison has a well-developed strategy to promote relationships and make sure women can fulfil any caring responsibilities.
Support to help women maintain contact with their family and friends had improved since our last inspection and now included an on-site social worker who provided advocacy and had important links to schools and children’s services.
The use of video visits (‘secure social video calling’; see Glossary) had increased, with calls available in the evenings during the week and during the day at weekends. Women could easily get help from Prison Advice and Care Trust (PACT; see Glossary) the family services provider, and monthly family days (see Glossary) took place. However, it was disappointing that, at the time of the inspection, only one woman was benefitting from ROTL to help maintain family ties.
Data was used well to identify prisoners who did not receive visits or phone calls, and they were invited to quarterly meetings in the visits hall, with attendance from New Bridge (see Glossary) which offered a pen pal service.
The environment in the visits hall was better than at our last inspection with more comfortable furniture and the addition of a small area with toys and books for younger children. However, some visitors had a poor experience on arrival as they had to wait in the rain without any cover before being allowed into the hall. Changes were being made to improve access to the family room, which allowed a private space for visits, and could be used for those with very young children or for sensitive conversations.
Living in the prison community
Expected outcomes: Women live in a prison which promotes a community ethos. They can access all the necessary support to address day-to-day needs and understand their legal rights. Consultation with women is paramount to the prison community and a good range of peer support is used effectively.
Consultation and support within the prison community
There was an impressive range of mostly well supervised peer workers who played a vital role in the running of the prison. Consultation with peer workers was regular but leaders had not extended this to other women.
Applications and complaints
| HMIP prisoner survey | Yes | Compared with the last inspection |
| Is it easy for you to make an application? | 60% | Higher |
The applications system remained unreliable, not helped by the lack of any technology on the house units or in cells. Paper application forms were not always available on the wings, and a new telephone system was not working as well as intended. Women calling were often unable to leave a voicemail message.
The number of complaints was reducing, and the system was generally managed well. Responses, in the sample we looked at, were polite and addressed issues raised, although not all were responded to on time.
Legal rights
Women had good support with their legal rights. The Not Beyond Redemption charity held monthly clinics giving free family law advice and representation. The Prisoners’ Advice Service ran regular sessions in the library, and there was adequate provision for legal visits but those held face-to-face were not sufficiently private.
Living conditions
Expected outcomes: Women live in a clean, decent and comfortable environment. They are provided with all the essential basic items.
Living conditions were reasonably good. All women lived in single cells which were furnished well; landings and association areas were generally clean; and hygiene products were readily available. Women had good access to outside areas which were pleasant and well maintained, particularly on D wing.



However, many of the residential units were old and dilapidated with much of the floor covering in need of replacement. Some wings were also very noisy, with staff shouting out when it was time for medication and the constant sound coming from the prison radios they carried.
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Normally, are these communal areas of your wing or houseblock very/quite clean: showers? | 57% | Lower |
While most showers had been refurbished, too few women said they were kept clean and many said that the water pressure was poor at times.
Women were able to get a haircut and could wash their underwear in a machine. Prison-issued clothing designed for women was available, but women described it as ill-fitting and poor quality.
In our survey, 57% of women said their cell call bell was answered within five minutes, which was better than at the two most similar prisons. Delays in response times were identified and discussed at daily leadership meetings to try to prevent this happening again.
Only 55% of women said they could use catalogues to buy what they needed. Access to stored property was also not good enough, and requests often got lost. More positively, an on-site shop selling black hair and beauty products had been introduced, better meeting the needs of this group of women.

| HMIP prisoner survey | Yes | Compared with similar prisons |
| Is the quality of the food in this prison very/quite good? | 43% | Lower |
| Do you get enough to eat at mealtimes always/most of the time? | 40% | Lower |
As in our survey, many women we spoke to were negative about the quality and quantity of the food. They said the menu was not changed often enough and provision for those with special dietary requirements was poor. Women were also concerned about the handling of halal food in the main kitchen. Leaders had been working to address these issues.
Health and social care
Expected outcomes: Women are cared for by services that assess and meet their health, social care and substance misuse needs and promote continuity of health and social care on release. The standard of health service provided is equivalent to that which women could expect to receive elsewhere in the community.
The inspection of health services was jointly undertaken by the Care Quality Commission (CQC) and HM Inspectorate of Prisons under a memorandum of understanding agreement between the agencies. The CQC found there were no breaches of the relevant regulations.
Strategy, clinical governance and partnerships
NHS England commissioners had effective contract monitoring arrangements. Central and North West London NHS Foundation Trust was the prime provider of health services. Dental care was provided by Time for Teeth. Psychosocial services were subcontracted to The Forward Trust.
The health care teams, the prison and key stakeholders worked in partnership, and they recognised the increased turnover of women and the growing complexity of their needs. Regular local delivery boards and much improved clinical governance structures ensured leaders had good oversight, and an improvement plan was in place.
Staffing levels were good, and health professionals were well trained. Supervision took place regularly and was recorded. Safeguarding arrangements were robust.
Health care complaints were low, and the service focused on early face-to-face resolution. Leaders had good oversight of reported incidents, and effective arrangements were in place to share lessons learned.
Clinical areas were clean and met infection prevention standards.
Promoting health and well-being
There was still no prison-wide health promotion strategy, but information materials were displayed across the prison. All new patients received a booklet outlining the available services and how to access them, however, these were only available in English. Health services did have access to a telephone interpreting service for appointments with non‑English speakers.
NHS age‑related health checks and preventative screening programmes were offered. Blood‑borne virus testing, immunisations and vaccinations were also available, and there were adequate contingency plans in place to manage potential outbreaks of infectious diseases.
There were no health peer workers, but plans were in place to address this.
Sexual and reproductive health (including mother and baby units)
A perinatal pathway was in place to provide multi‑agency oversight should the need arise. Support was offered to women who had experienced a pregnancy within the previous two years including loss through termination, miscarriage, or separation. Additionally, they had good access to counselling services.
A sexual health consultant provided a comprehensive monthly service, offering a full range of treatment, support and advice for women during their stay and through the gate on release. Women who required testing for sexually transmitted infections were able to complete self‑testing in the privacy of their own cell, which was a positive feature of the service.
Staff provided clear information about the importance of having cervical smear tests and had introduced ways of reducing anxiety, including the use of chaperones at appointments if requested.
Primary care and enhanced units (inpatients and well-being units)
Patients we spoke to said health care provision was good. They had access to a positive range of services. New arrivals were assessed in reception with secondary screening undertaken within seven days. Services were available seven days a week, and overnight NHS 111 or urgent care was used. Wait times to see a GP were reasonable at no more than six days. The clinical day was until 8pm which reduced late arrivals being missed until the next day.
Patients with long term conditions spoke of feeling cared for, but some plans and the management of long-term conditions was unacceptable. Poor use of clinical recording and lack of face-to-face care planning in some instances meant these patients were not well monitored. The lack of a long-term condition nurse was impacting overall care for those with complex health conditions.
Emergency responses were promptly attended by nurses with appropriate equipment. Emergency equipment was kept on each wing and checked regularly.
There was a range of visiting practitioners and allied health care professionals and waiting times for their services were reasonable.
Most hospital escorts went ahead as planned with only a small number of appointments cancelled. Administrative staff kept in regular contact with hospitals to ensure that patients received an appointment date when referrals were made.
Mental health
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Do you have any mental health problems? | 80% | No difference |
The well‑led and highly regarded team delivered a good standard of evidence‑based care to respond to the high level of mental health need. Referrals came from various sources, were triaged effectively and allocated appropriately. Most waiting times were reasonable but were longer for psychological therapies.
Staffing levels had increased, with an impressive range of experienced disciplines, but suitable space for individual and group therapies was limited. Clinical staff were visible across the prison, attended segregation and all initial ACCT reviews, and safety meetings.
Access to psychiatry was prompt, with effective arrangements for reviewing the physical health of patients on medication. A neurodiversity assessment and treatment pathway was in place, and the prison neurodiversity manager was co‑located with the mental health team.
Patients spoke positively about the support received and, in our survey, one woman wrote:
“My mental health worker has been brilliant; the whole team are helpful and kind. I wouldn’t have got through without them.”
Care planning, risk management and physical health monitoring were effective, and clinicians arranged appropriate aftercare on transfer or release.
| Data provided by the prison | Time period | |
| Number of patients transferred to hospital under the Mental Health Act | 13 | 12 months prior to inspection |
Leaders reported more women arriving acutely mentally unwell, often close to their release date. Despite a large increase in the number needing treatment in hospital under the Mental Health Act, outcomes remained extremely poor for them. Most waited over 28 days, and in one case, it took 154 days to find an available bed space. While awaiting transfer many were held in the segregation unit at the prison, which was wholly unacceptable.
Social care
Surrey County Council (SCC) and the prison had a memorandum of understanding setting out how social care would be provided. SCC staff attended the weekly induction session for newly arrived women, which was positive. Anyone could make a referral, including women and their families, and they were assessed promptly.
Care plans were detailed, and at the time of inspection three women were receiving care. They spoke positively about the support and had been given a copy of their plan. Suitable aids and equipment were provided to help them manage daily living tasks.
Two peer carers supported women with lower‑level needs and were trained and supervised by SCC staff. However, SCC staff did not record this support on the electronic health record, SystmOne.
Substance misuse and dependency
All new arrivals had good access to psychosocial and clinical substance misuse treatments. Services were well integrated, working closely with other departments and the prison. Psychosocial provision included additional roles, such as a family worker.
Clinical notes and care plans were personalised with reviews taking place at the required intervals. Women felt involved in decisions about their care. However, The Forward Trust continued to use separate clinical notes, which posed a risk.
A dedicated clinical team supported women on opioid substitution treatment (OST). At the time of inspection, 48 women were on OST, with 14 receiving long‑acting buprenorphine injections. Women on this medicine reported improved functioning and well-being.
Women had access to groups facilitated by the psychosocial team, with credible plans to expand these. Mutual aid groups such as Alcoholics Anonymous and Narcotics Anonymous visited regularly.
An incentivised substance free living wing was highly valued by residents. However, some women on OST were not reducing, which did not align with the wing’s intended ethos.
Continuity of care on release was strong. Timely referrals were made to community services, prescriptions were arranged in advance, and women received harm‑reduction information, naloxone training and supply.
Medicines and pharmacy services
Governance was good overall. All clinical prescriptions were screened and prescribing trends were monitored. There was strong oversight of tradeable medicines, and the team participated in the regional medicines management group.
There was good access to a wide range of medicines, dispensed safely and on time. Wing‑based administration was well managed, with good officer supervision of queues. Administration in segregation was unsafe, but leaders rectified this immediately.
Medicines reconciliation took place promptly after arrival, with effective arrangements to obtain urgent and critical medicines.
Patients had good access to the pharmacist for medicines reviews, and joint working with primary care ensured appropriate pain relief prescribing. All medicines were supplied as patient‑named items with appropriate labelling and audit trails. There was adequate out‑of‑hours provision, and women could now buy simple pain relief from the canteen.
Adherence was monitored, and concerns such as poor compliance or suspected diversion were addressed promptly. Around 65% of women received medicines in‑possession, supported by up‑to‑date risk assessments. Random spot checks were conducted regularly.
Dental and oral health
A permanent dental team was on site three days a week, and waiting times were not excessive at about four to five weeks on average for a routine appointment.
The treatment room and separate decontamination area were clean and met infection control standards. Equipment was maintained and serviced to ensure it was safe and fit for purpose.
Governance was maintained with accurate digital, paper and record keeping documentation available.
Fair treatment and inclusion
Expected outcomes: There is a clear approach to promoting equality of opportunity, eliminating discrimination and fostering good relationships. The distinct needs of prisoners with protected characteristics, or those who may be at risk of discrimination or unequal treatment, are addressed. Women are able to practise their religion and the chaplaincy plays a full part in prison life, contributing to women’s overall care, support and rehabilitation.
Leaders were visible and approachable, and strong key work and peer support meant that prisoners from different groups could have their voices heard. However, formal consultation did not take place regularly and failed to lead to meaningful change. The quality of discrimination incident reporting form (DIRF; see Glossary) responses was too variable, however, plans were in place to improve staff training and provide external scrutiny.
The new equalities manager had improved the use of data to begin to identify and understand disproportionate outcomes. However, some women we spoke to described discriminatory treatment, including inappropriate attitudes or responses from some staff.
The prison-based social worker connected care leavers with their local authority personal advisors to make sure they received the help to which they were entitled.
The needs of prisoners who did not speak English well were not being met. Telephone interpreting was rarely used, including during health care consultations, and there was insufficient written material around the prison to explain the basics of prison life.
An on-site shop selling black hair and beauty products had been introduced, which was valued by women.
Transgender prisoners received respectful treatment and had access to appropriate clothing and personal items.
Accessibility around the site for women who used a wheelchair was good overall, and social care adaptations were made when needed. Support for deaf prisoners had been introduced, such as using British Sign Language interpreters and whiteboards to provide visual communication.
There were some good initiatives to support neurodivergent prisoners. This included the addition of group-based interventions aimed at helping them to cope in prison. Neurodivergency passports were used to help staff understand behaviour and tailor their communication. Additional training on neurodivergency for operational staff was planned.
Faith and religion
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Have you spoken to the chaplaincy team in this prison? | 89% | No difference |
| For those who have a religion: Are your religious beliefs respected here? | 65% | No difference |
The chaplaincy team delivered an impressive range of interventions to support women, including bereavement counselling, and 93% of those we surveyed said they could access religious services.
It was unusual to receive negative feedback regarding the chaplaincy, but some women described serious grievances about the quality of individual support, including one example of arrangements to attend a funeral not being put in place.
Section 4: Purposeful activity (Back to top)
Women are able and expected to engage in activity that is likely to benefit them, including a positive range of recreational and social activities.
Time out of cell, recreational and social activities
Expected outcomes: All prisoners have sufficient time out of cell (see Glossary) and are encouraged to engage in recreational and social activities which support their well-being and promote effective rehabilitation.
| HMIP time out of cell data (at the time of the inspection) | |
| Average proportion of prisoners locked up during the working day | 16% |
Time out of cell for most prisoners was reasonably good. Our roll checks found that 64% of the population were engaged in education, work or training off their unit, and prison data showed that 90% were employed full-time, which included women working on the wing. Most of these prisoners had just over 11 hours out of cell each day from Monday to Thursday.
However, unemployed prisoners and those on the lowest level of the incentives scheme only got 2.5 hours out of cell each day during the week. Most women were also locked in cell for too long on a Friday and over the weekend.
Almost all women knew what the lock up and unlock times were supposed to be and the regime was delivered reliably. Access to outside exercise, domestic periods and association time was good for most prisoners.
Some recreational and social activities were available, including Parkruns, gym sessions and a prison choir.
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Are you able to visit the library once a week or more? | 76% | Higher |
Access to the well-stocked library was good and our survey results were positive. However, it was only open four days a week, and technical problems with the system used for issuing books caused long delays and frustrations. Activities and events to promote reading were provided with popular initiatives including the monthly book club, a ten-week philosophy course, and the Reading Ahead programme.

Despite shortages of PE staff, 86% of respondents in our survey said they were able to attend sports or gym sessions at least once a week, however, weekend provision was more limited. Gym equipment was modern, and women could participate in a variety of activities including yoga, coaching and individual training plans, which helped some to achieve health and fitness goals.


Education, skills and work activities
Expected outcomes: All women are expected and enabled to engage in education, skills or work activities that increase their employability on release. There are sufficient, suitable education, skills and work places to meet the needs of the population and provision is of a good standard
Ofsted inspects the provision of education, skills and work in custodial establishments in England. The following summary has been provided by Ofsted inspectors who attended this inspection. Their full report is published under ‘Further resources’.
Ofsted made the following assessments about the education, skills and work provision:
- Overall effectiveness: Good
- Quality of education: Good
- Behaviour and attitudes: Good
- Personal development: Good
- Leadership and management: Good
Leaders had rectified the concerns raised at the previous inspection. They had ensured that women received helpful advice and guidance when choosing their education, skills and work activities. Staff mostly provided high-quality feedback to help women improve their work. They provided individual help and support to women so that they could catch up on any lost learning.
Leaders provided sufficient purposeful activities spaces for women to join education courses and develop their skills. Staff allocated spaces thoughtfully, matching activities to women’s individual interests and potential employment routes. Almost all activity spaces were allocated and most women attended on a full-time basis. Women attended well and were mostly punctual.
Leaders provided a broad employment-focused curriculum, designed for women to develop the knowledge, skills and behaviours they needed to secure work both before and after release. Leaders had carefully curated a series of pathways that covered a wide range of sectors including retail and business enterprise, as well as practical skills such as gardening and sustainability.
Leaders had responded quickly to changing population needs, creating a pathway for women approaching release that helped them to build employability skills rapidly. Staff focused appropriately on improving women’s confidence and self-esteem in accredited and non-accredited courses, including those in construction and recycling. Leaders prioritised essential work-ready behaviours such as attendance, time-keeping and mutual respect.
Leaders worked effectively with staff from Milton Keynes College to provide high-quality education and training for women studying education courses such as English, mathematics and beauty therapy. Almost all women passed their courses and achieved their qualifications.
In subjects such as mathematics and English, staff set useful targets that helped women to track their progress. However, in a minority of business-critical work functions, such as kitchens, gardens and wing work, progress recording was weaker. Staff in these areas did not routinely set targets that were sufficiently challenging or relevant to the skills women were expected to develop.
Staff promptly identified women who needed support with reading, working with the Shannon Trust (see Glossary) to offer appropriate help on the wings and in lessons. Leaders recognised they needed to improve book choice and presentation in areas such as workshops and residential units.
Staff used partnerships with external organisations, including the London College of Fashion, Max Spielman and The Clink, to provide women with experience of working in industry settings and commercial kitchens. Training was strongly employment-focused, enabling women to build skills, such as pattern making and catering for events, that they could use both on ROTL and future work.
Staff consistently identified any special educational needs and/or disabilities and provided useful strategies that supported women effectively. Women with additional needs achieved at the same high rate as their peers.
Despite some excellent opportunities for ROTL, only two women were accessing this at the time of the inspection. Those who had been granted ROTL previously had made good progress and secured employment on release.
Staff provided women with helpful and supportive careers information, advice and guidance to help them understand the range of options available to them.
Staff taught women how to spot the signs of radicalisation and extremism risks as part of induction. The dangers of radicalisation and extremism were further embedded within education classes and staff had received specific training to identify issues of concern. However, this was not reinforced sufficiently well so that women could recall fluently how to spot the signs in themselves and others.
Section 5: Preparation for release (Back to top)
Preparation for release is understood as a core function of the prison. Women are helped to reduce their likelihood of reoffending and their risk of harm is managed effectively. Women are prepared for their release back into the community.
Reducing reoffending
Expected outcomes: Women are helped to change behaviours that contribute to offending. Staff help them to demonstrate their progress.
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Do you think your experiences in this prison have made you less likely to offend in the future? | 60% | No difference |
Around two-thirds of the population were serving sentences of more than four years, in addition to an increase in the number serving life. These women could access activities and interventions tailored to their need to progress.
The makeup of the remaining population had changed significantly since our last inspection, with more prisoners assessed as high risk of harm to others; more arriving with only a few months left to serve; and a huge increase in the number of releases. However, services had not been fully adapted to meet this new level and type of need.
The OMU was chronically short staffed. This led to basic tasks such as sentence calculation, assessment for release on home detention curfew (HDC; see Glossary) and ROTL being delayed, which frustrated many prisoners. About 60 recategorisation reviews were overdue, and some were months late. Nonetheless, it was good to see that nearly 50 women had moved to open conditions in the last year.
The OMU team was short of one part time probation manager and had too few probation officers to manage the number of high risk women. Nevertheless, we were impressed by the team of prison offender managers (POMs), who knew women extremely well and were knowledgeable about risks, vulnerabilities and public protection concerns. We saw examples of them working hard to provide excellent help to some vulnerable women.
However, POMs typically did not have time for ongoing, meaningful one-to-one work with women. While those serving long sentences could benefit from therapeutic support alongside valuable employment opportunities, the frequency of POM contact with them was limited. Despite this, our survey showed that 83% of women knew what their objectives or targets were, and 78% understood what they needed to do to achieve them.
Opportunities for women to progress
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Has the prison allocated you to the education, training or work that will help you when you are released? | 69% | Higher |
Women had good opportunities to progress, including an impressive range of education and training that would help them on release, alongside other interventions such as those helping with mental health or substance misuse problems (see Mental Health and Substance misuse and dependency). In our survey, one prisoner wrote:
“…I am clean and look forward to staying clean… I was able to address my problems to the full extent here… this prison really helped me see things differently and I really can see my future being clean and sober.”
Although there was a good focus on improving employment opportunities with solid links to employers, there was hardly any use of ROTL.
Options, part of the joint NHS/HMPPS national Offender Personality Disorder Pathway (see Glossary), was excellent and provided help to some high-risk prisoners with complex needs through individual and group therapy as well as one-to-one support sessions. Prisoners gave us specific examples of how this course had benefited their well-being, thinking and behaviours.
Help for those who had experienced loss and bereavement was good. One-to-one counselling was available, and data from the prison over the three months before our visit showed that, after completion, women reported lower levels of anxiety and depression.
Delivery of the new accredited programme, Building Choices, had been slow with only four prisoners completing it since November 2025. Ongoing staffing problems meant the team was unlikely to offer it to all who needed it.
The psychology team worked closely with the OMU to identify prisoners who may have risks or needs that needed addressing through other interventions. They delivered individualised risk reduction work and provided some progression work to prisoners convicted of sexual offences.
Returning to the community
Expected outcomes: Women’s specific reintegration needs are met through good multi-agency working to maximise the likelihood of successful resettlement on release.
| Data provided by the prison | |
| Number of releases in the 12 months leading up to our last inspection | 159 |
| Number of releases in the 12 months leading up to this inspection | 508 |
The number of releases had increased considerably since the last inspection, yet there were no more resources allocated to resettlement planning and support, apart from the addition of a support worker to help women apply for identification documents and open bank accounts.
Responsibility for release planning largely fell to the already extremely stretched POMs, who spent much of their time either confirming arrangements with community probation teams across the country or stepping in themselves to put plans in place. Some release support, including those for high risk and MAPPA-eligible prisoners (multi-agency public protection arrangements; see Glossary), was precarious and was only agreed at the last minute.
The lack of accommodation for high-risk and vulnerable women had resulted in some poor outcomes. For example, during the inspection, a high-risk prisoner without a confirmed MAPPA management level had offers of places at two different approved premises withdrawn just before her release day. A bed in another approved premises was only secured through the determined efforts of POMs while the prisoner waited in reception on the morning of release. After all this confusion, the prisoner never reached the hostel and was subsequently recalled.
Less than a quarter of released women had sustainable accommodation to go to, and about 10% were homeless or failed to attend housing that had been arranged for them.
There was nowhere outside the gate for women to meet resettlement agencies or plan their onward journeys following their release, and there was little ‘through the gate’ support from community-based agencies. Positively, OMU staff would book the National Rail passenger assist service for the most vulnerable women travelling long distances, so they would be identified by railway staff at the start of their journeys and supported to change trains and reach their destinations.
Section 6: About HMP & YOI Downview (Back to top)
Category of the prison
A women’s closed training prison.
Brief history
HMP Downview first opened in 1989 as a category C men’s prison. In 2001, it was converted into an establishment for women. However, in 2013, the Ministry of Justice (MoJ) announced its intention to turn it back into a men’s prison. Shortly afterwards, it closed for two years and eight months. Following the closure of HMP Holloway, it was decided to retain Downview within the women’s estate. The prison reopened in May 2016.
Population
- 302 women were held at the time of the inspection with an operational capacity of 356.
- On average, there had been 47 new receptions each month.
- In the last 12 months, 508 women had been released into the community.
- 139 people were receiving support for substance misuse at the time of the inspection.
- 20–25 prisoners had been referred for mental health assessment each month.
Short description of residential units
A wing – induction unit, including peer workers
B wing – general population
C wing north 1 & 2 – incentivised substance free living (ISFL; Glossary)
C wing south 1 & 2 – enhanced population
C wing 3 & 4 – enhanced and general population
D wing – resettlement and peer mentors
E wing – unit for transgender women
Prison status (public/private)
Public
Key providers
Physical health provider: Central and North West London NHS Foundation Trust
Mental health provider: Central and North West London NHS Foundation Trust
Substance misuse treatment provider: Forward Trust
Dental health provider: Time for Teeth, subcontracted to Central and North West London NHS Foundation Trust
Prison education framework provider: Milton Keynes College
Escort contractor: Serco
Prison group director
Carlene Dixon
Name of governor/director and date in post
Amy Dixon, June 2022
Changes of governor/director since the last inspection
Natasha Wilson, December 2018 – April 2022
Date of last inspection
12–23 July 2021
Progress on concerns from the last inspection (Back to top)
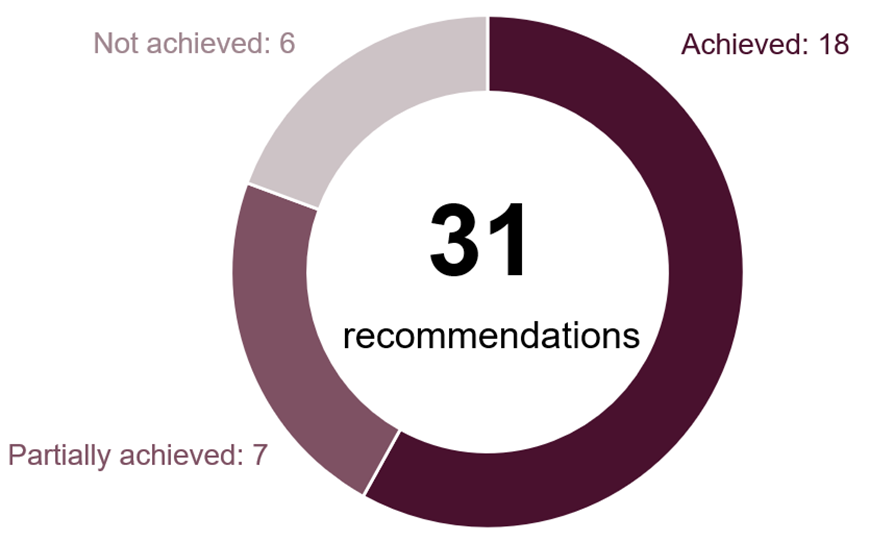
At our last inspection in 2021 we made 31 recommendations, five of which were about key areas of concern.
At this inspection we found the following progress:
The following is a list of all the recommendations raised, organised under the four tests of a healthy prison.
Safety
Key recommendations
Staff’s relationships with women should reflect a rehabilitative and trauma-responsive approach.
Partially achieved
Recommendations
A strategy and action plan should be developed to provide effective oversight of the level of self-harm and to reduce its incidence.
Partially achieved
Adult safeguarding work should be promoted through training for staff and links with the local authority.
Achieved
The incentives scheme should reward positive behaviour and motivate women.
Partially achieved
Use of force incidents should be effectively recorded and monitored, as well as regularly scrutinised.
Achieved
There should be a multidisciplinary approach to reducing the drug supply that links with a demand reduction strategy.
Achieved
Respect
Key recommendations
The prison should ensure that women receive sufficient support to help them maintain and develop positive relationships with their children, family members and other people significant to them.
Achieved
Local partners and prison leaders should use the local quality and delivery board and contracts meetings to improve communication and consultation. Assurances that health services are effective should be sought, including ensuring sufficient staff to escort women to their appointments.
Achieved
Enough clinically qualified staff should be available every day to oversee patient applications, electronic tasks, the GP waiting list and long-term conditions, to optimise women’s health outcomes.
Achieved
Recommendations
Women should have confidence in the complaints process, which should be effective, timely and appropriately managed.
Partially achieved
Women should be able to access their stored property promptly.
Not achieved
An overarching health promotion strategy should be established to support women to improve their health and well-being.
Not achieved
Women should have access to appropriate psychological interventions to meet their identified mental health needs.
Achieved
Medicines should be administered at the right times for optimum therapeutic effect.
Achieved
Women should have the same access to paracetamol as they would in the community.
Achieved
Women given medication to hold in their possession should be monitored regularly to be sure this remains safe, especially following their transfer to the prison.
Achieved
The prison should produce, regularly review, and act on, up-to-date equality data
Achieved
Women with protected and minority characteristics should be consulted regularly to ensure their individual needs are met.
Partially achieved
Muslim prisoners should be able to attend services in the chapel or multi-faith room.
Achieved
Purposeful activity
Key recommendations
The prison should improve consultation and communication to ensure women and staff are aware of changes that affect their daily lives.
Achieved
Recommendations
Indoor association should be resumed and should offer women a range of social and recreational activities, facilities and equipment.
Partially achieved
Gym provision should be extended into the evenings, particularly for those working during the day.
Partially achieved
Leaders and managers must make sure that women retain and reinforce their knowledge. They should introduce strategies to help women catch up with lost learning when planning their return to face-to-face lessons and work areas.
Achieved
Leaders and managers must make sure that women receive helpful advice and guidance so that they feel well-informed when choosing their education, skills and work activities.
Achieved
Leaders and managers should make sure that staff provide feedback on women’s work that helps them to improve and assist those engaged in work activities with any learning needs.
Achieved
Resettlement
Recommendations
The reducing reoffending strategy and action plan should be in place to drive improvement and ensure evidence of success can be recorded.
Achieved
The oversight and coordination of the range of interventions available across the prison should be improved and communicated to relevant staff and women.
Achieved
All OASys documents should be up to date.
Not achieved
The prison should make better use of ROTL for education or for paid or voluntary work placements.
Not achieved
Prison officer operational POMs should have sufficient time to work consistently and support women on their caseloads.
Not achieved
Women serving long or indeterminate sentences should receive appropriate advice and support to enable them to progress in custody.
Not achieved
More about this report (Back to top)
This report outlines the priority and key concerns from the inspection and our judgements against the four healthy prison tests. Each of the following four sections contains a detailed account of our findings against our Expectations for men’s prisons.
Find out more about our Expectations and how we inspect
Find out more about priority and key concerns
Find out about notable positive practice
Findings from the survey of prisoners and a detailed description of the survey methodology are published alongside this report. Please note that we only refer to comparisons with other comparable establishments or previous inspections when these are statistically significant. The significance level is set at 0.01, which means that there is only a 1% chance that the difference in results is due to chance.
The tables in this report which provide data from HMI Prisons prisoner surveys also include comparisons with similar prisons.
| Description | What it means |
| Lower | the prison’s percentage is statistically significantly lower than the comparator: prisons with the same function type, or at the last inspection |
| Higher | the prison’s percentage is statistically significantly higher than the comparator: prisons with the same function type, or at the last inspection |
| No difference | the prison’s percentage is not statistically significantly different to the comparator: prisons with the same function type, or at the last inspection |
Inspection team
This inspection was carried out by:
| Charlie Taylor Sandra Fieldhouse Jessie Wilson Kellie Reeve Rebecca Stanbury Jonathan Tickner John Wharton Helen Ranns Alicia Grassom Emma Crook Sana Zahid Shaun Thomson Lynn Glassup Mark Griffiths Sarah Alexander Matt Hann Chris Dearnley | Chief inspector Team leader Inspector Inspector Inspector Inspector Inspector Researcher Researcher Researcher Researcher Lead health and social care inspector Health and social care inspector Care Quality Commission inspector Ofsted inspector Ofsted inspector Ofsted inspector |
Further resources (Back to top)
These files may not be suitable for users of assistive technology.
Request an accessible format
If you use assistive technology (such as a screen reader) and need a version of any of these documents in a more accessible format, please email media@hmiprisons.gov.uk. Please tell us what format you need. It will help us if you say what assistive technology you use.
Find out more about the terms and abbreviations used in this report in our glossary.