
HMP Isle of Wight
Report on an unannounced inspection of HMP Isle of Wight by HM Chief Inspector of Prisons 16–26 March 2026.

Introduction (Back to top)
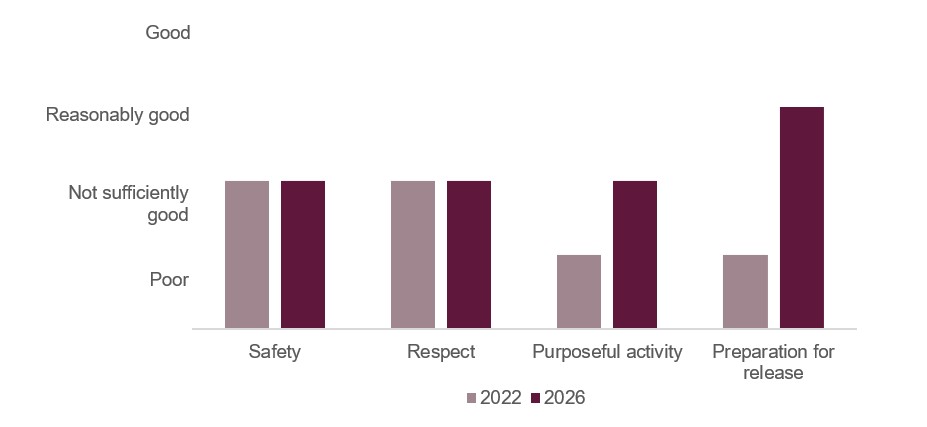
While some healthy prison assessment scores had improved on this inspection, Isle of Wight continued to be a jail that significantly underperformed with a lack of meaningful incentives for the many prisoners who behave well, a poor regime, frequent staff shortages and insufficient suitable workshop spaces for the population. Leaders were not helped by a sprawling, ageing site, particularly the Albany side that is simply not fit for purpose. The scores in our tests for safety and respect remained ‘not sufficiently good’, but purposeful activity and preparation for release, both rated as ‘poor’ last time, had improved to ‘not sufficiently good’ and ‘reasonably good’ respectively.
The prison was in the process of taking on a greater proportion of category B prisoners convicted of sexual offences, some of whom were serving very long or indeterminate sentences. In our survey 56% of prisoners told us that drugs were easy to get; a large increase on our last inspection. There had also been an increase in rates of violence since our last visit. The prison service had not profiled for this change in population, and the governor had needed to cross-deploy staff into the segregation unit in order to be able to keep prisoners and officers safe. Designed originally as a high-security provision, conditions on the unit were poor, with some men spending long periods of time with a very limited regime that, when the unit was full, meant they could only shower every other day.
Leaders had increased the number of supervising officers; these and other temporary promotions left vacancies among prison officers. This led to frequent regime curtailments and our checks showed that a third of prisoners were locked behind their doors. The regime was not adequate for a training prison which was not getting enough men into education or workshops, many of which were closed because of difficulty recruiting trainers. While attendance at workshops was reasonably good, it was unacceptably poor in education.
Rates of self-harm remained among some of the highest in all prisons and although leaders had begun to put more support in place, they had not done enough to address or understand some of the underlying causes such as debt and the limited regime. Mental health support for those with the most serious illness was reasonably good, but staff shortages meant that many men did not get adequate care.
Health care provision had improved, but governance was not tight enough and there was a very limited offer for the many prisoners with addiction problems.
Although cells were generally well looked after, the infrastructure and buildings in both sites were poor. Landings and stairways were dirty and many showers were in disrepair. Absurd MoJ procurement rules meant it had taken far too long for the governor to be able to purchase replacement washing machines.
On the Albany site things were particularly bad with night sanitation still operating. This was not decent, particularly for an ageing population and those with mobility issues who only had seven minutes to use the lavatory before they were locked away again. This had led to prisoners resorting to using buckets in their cells, the contents of which were often then tipped out of the windows.
While recruiting sufficient probation staff remained a serious problem, the hardworking and impressive senior probation officer and the psychology teams had put creditable effort into creating a much more rehabilitative environment than at our last inspection. Public protection arrangements were now much better and staff were working hard to keep sentence plans and release preparation up to date. An impressive ‘trauma informed’ wing was supporting some very complex men with beginning to understand and address their offending. Disappointingly, elsewhere in the prison there were not nearly enough incentives to encourage prisoners to behave. The many prisoners who were on an enhanced regime, complained that they could earn few privileges.
The well-regarded, long-serving governor had worked hard with his senior team to stabilise the prison and make preparations for a changing population. They will need to make sure that health care continues to improve to support the many older and vulnerable prisoners. There will also need to be a concerted effort to improve the range of activities and develop the regime and to be more imaginative about how to incentivise prisoners to behave well. The prison service must improve the staffing profiles in this complex site, and fund improvements in the infrastructure and buildings, so that this category B training prison can begin to really fulfil its function.
Charlie Taylor, HM Chief Inspector of Prisons, May 2026
Outcomes for prisoners (Back to top)
We assess outcomes for prisoners against four healthy prison tests: safety, respect, purposeful activity, and preparation for release (see More about this report for more information about the tests). We also include a commentary on leadership in the prison (see Section 1).
At this inspection of HMP Isle of Wight we found that outcomes for prisoners were:
- not sufficiently good for safety
- not sufficiently good for respect
- not sufficiently good for purposeful activity
- reasonably good for preparation for release
We last inspected HMP Isle of Wight in 2022. Figure 1 shows how outcomes for prisoners have changed since the last inspection.
Figure 1: HMP Isle of Wight healthy prison outcomes 2022 and 2026
What needs to improve (Back to top)
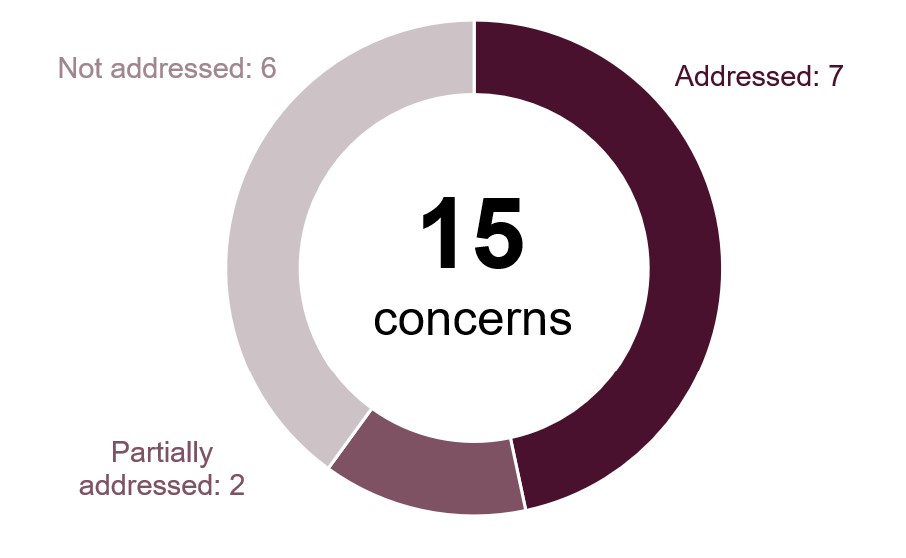
During this inspection we identified 15 key concerns, of which six should be treated as priorities. Priority concerns are those that are most important to improving outcomes for prisoners. They require immediate attention by leaders and managers.
| Priority concerns | |
| 1. | Governance and oversight of important areas, including segregation and adjudications, were weak, and data were not used well to drive improvements. |
| 2. | Self-harm remained high and was the fifth highest of all adult male prisons. |
| 3. | Infrastructure was failing across both sites and insufficient investment had been made by HMPPS to remedy this. |
| 4. | Health leadership oversight and scrutiny of some areas of the governance framework, including incident reporting, audit, complaints and aspects of record keeping, were poor. |
| 5. | Leaders had not made sure that prisoners were consistently allocated to sufficient and purposeful education, skills and work activities. |
| 6. | Prisoners had insufficient contact with prison offender managers which did not support sentence progression. |
| Key concerns | |
| 7. | There was too little to incentivise prisoners to behave, and both violence and illicit drug use had increased. |
| 8. | Use of force had increased and scrutiny was weak. |
| 9. | Oversight of decency and cleanliness of residential units was insufficient, and the electronic night sanitation system was indecent and unhygienic. |
| 10. | Work to promote fair treatment had not been sufficiently prioritised. Leaders had not acted on data showing disproportionate outcomes for some groups, and consultation with prisoners from protected characteristic groups was limited and ineffective. |
| 11. | Patients waited too long to be transferred under the Mental Health Act for assessment or treatment in a mental health unit, breaching the 28-day transfer guideline. |
| 12. | Substance misuse and mental health teams delivered insufficient one-to-one and group interventions across both sites. |
| 13. | Leaders’ oversight and use of data did not sufficiently evaluate participation and improve the quality of education, skills and work. |
| 14. | Prisoners spent too long locked up. The regime was poor for those not engaged in purposeful activity, including the retired and sick. |
| 15. | Leaders had not established a sufficiently developed or coherent personal development curriculum. |
Notable positive practice (Back to top)
We define notable positive practice as evidence of our expectations being met to deliver particularly good outcomes for prisoners, and/or particularly original or creative approaches to problem solving. Inspectors found seven examples of notable positive practice during this inspection, which other prisons may be able to learn from or replicate.
| 1. | Databases for recording and tracking paper-based applications and all catalogue orders were useful and provided good oversight (see Prisoner consultation, applications and redress). |
| 2. | The ‘settlement’ programme delivered jointly by staff and prisoners provided a well‑structured and comprehensive induction to prison life (see Early days in custody). |
| 3. | The gym timetable offered an impressive range of activities seven days a week to meet the needs and preferences of the diverse population (see Time out of cell). |
| 4. | Leaders had established a highly inclusive and particularly effective reading strategy that engaged prisoners with diverse needs (see Education, skills and work activities). |
| 5. | Regular on-line and face-to-face visitor forums held by leaders helped to improve the overall visitor experience (see Children and families and contact with the outside world). |
| 6. | The dedicated unit for prisoners with a history of trauma provided a community to help men understand and address offending behaviours (see Opportunities for prisoners to progress). |
| 7. | Prisoners were able to complete a resettlement course based on the needs of men returning to the community after long sentences (see Returning to the community). |
Unless otherwise specified, these examples are not formally evaluated, are a snapshot in time and may not be suitable for other establishments. They show some of the ways our expectations might be met, but are by no means the only way.
Section 1: Leadership (Back to top)
Leaders provide the direction, encouragement and resources to enable good outcomes for prisoners.
The longstanding and experienced governor had a clear vision for the prison and gave an honest assessment of its strengths and weaknesses. Senior leaders had responded to local staff surveys highlighting a lack of trust in leadership through a range of actions that included increasing their visibility.
Senior leaders were taking appropriate action to manage the transition to holding a population of category B prisoners. This included strengthening the supervisory tier by increasing Band 4 roles to support and build officers’ confidence.
However, there were not enough officers to manage the demands of the more complex population, leading to reports of low staff morale and frequent regime curtailments. Staffing difficulties were compounded by a quarter being unavailable for operational duties because of high levels of temporary promotion and sickness absence.
While there were gaps in training for staff working with prisoners convicted of sexual offences, there had been efforts at upskilling, for example to increase understanding of offending behaviour programme objectives and improve security practices. Training was also offered to new managers, although the capability of middle leaders remained variable.
Leaders had not done enough to provide suitable full-time purposeful activity for the population following HMPPS changes to workplace risk assessments which had increased the number of prisoners deemed ‘high risk’. Management of activity allocation and attendance was also not good enough, and too many prisoners spent far too long locked up for a training prison.
Although HMPPS funding for some enhanced gate security was agreed, there had been insufficient investment in failing infrastructure across both sites. While leaders had driven some improvements in living conditions, most units remained worn and shabby, and the night sanitation arrangements in Albany were indecent and unhygienic.
Despite ongoing difficulty recruiting probation officers, leadership of the offender management unit (OMU) had improved since the previous inspection, and there was now a prison-wide focus on public protection.
Leaders in key areas such as activities, health care and equality were still not using data effectively to drive improvements. We also found gaps in assurance and oversight, particularly within the safety function.
The work of the psychology team was well integrated and the rehabilitative ethos of the ‘trauma-informed’ unit was very strong. However, more needed to be done to replicate this approach across both sites. Leaders’ plans to introduce a ‘Steps to Positive Change’ strategy to support sentence progression for the largely long-term population were encouraging.
Section 2: Safety (Back to top)
Prisoners, particularly the most vulnerable, are held safely.
Early days in custody
Expected outcomes: Prisoners transferring to and from the prison are safe and treated decently. On arrival prisoners are safe and treated with respect. Risks are identified and addressed at reception. Prisoners are supported on their first night. Induction is comprehensive.
Around seven new prisoners arrived each week, most of whom had had long journeys to reach the prison. There was also a small local remand population.
In our survey, 91% of prisoners said they were treated well in reception. However, oversight of early days was weak; staff were unclear about their responsibilities and records were incomplete. This created risk that potential vulnerability was not always identified or acted upon.
Cells for new arrivals were not always adequately prepared. In our survey, only 28% said they were offered a shower on their first night, and just 43% said they could get pin phone credit in their first few days.
Prisoners convicted of sexual offences (PCOSOs), who comprised the majority of the population, received a comprehensive induction which covered helpful topics including debt management, how to cope when struggling, health and hygiene, as well as activities.
However, there was no formal induction for those on remand. They also spent too much time locked up.
Promoting positive behaviour
Expected outcomes: Prisoners live in a safe, well ordered and motivational environment where their positive behaviour is promoted and rewarded. Unacceptable conduct is dealt with in an objective, fair, proportionate and consistent manner.
Encouraging positive behaviour
| HMIP prisoner survey | Yes | Compared with last inspection |
| Do you currently feel unsafe? | 25% | No difference |
Rates of violence had increased since our last inspection and were on an upward trajectory.
The recently developed safety strategy had identified debt, illicit substances and bullying as the main drivers behind violence, and prisoners we spoke to confirmed this. A debt strategy was being developed but leaders still needed to do more to understand how they could support prisoners.
All incidents of violence were referred for individual case management through challenge, support and intervention plans (CSIPs, see Glossary) and investigated in reasonable time frames. Plans and targets were not always meaningful, although for some of the most complex prisoners, there was good evidence of multidisciplinary working and input from a psychologist.
There was no process to investigate why prisoners chose to isolate for their own safety, monitor their regime or support their reintegration with the rest of the population.
Although the enhanced unit on the Parkhurst site provided a good incentive, poor time out of cell and few enrichment activities meant there was little to motivate the rest of the population. Many enhanced prisoners told us that they did not feel there was any benefit in achieving the highest level of incentive regime status.
There had been an increase in adjudications since the previous inspection, many of which related to violent incidents and the illicit economy. At the time of the inspection, 138 adjudications remained unresolved, reducing the overall effectiveness of the process. However, the recent appointment of a crime-in-prisons co‑ordinator was enabling progress with cases requiring police involvement.
Oversight of adjudications had lapsed, with no scrutiny meetings held in recent months. Leaders had recently started quality assurance of adjudication records to address this gap.
Use of force
| Data provided by the prison | |
| Number of uses of force in the 12 months before this inspection | 826 |
| Number of uses of force in the 12 months before the last inspection | 242 |
Use of force rates had increased since the last inspection. but a large proportion was low level and around 40% of incidents involved the use of handcuffs to escort prisoners subject to additional safety measures. PAVA (see Glossary) and batons had not been used in the last year.
Governance of force was weak; monthly meetings had not taken place regularly and weekly scrutiny meetings had only very recently started. Incidents were being triaged by use of force instructors, but there was a backlog of around a month because staff were frequently redeployed.
The incident footage that we reviewed showed that use of force was generally proportionate and reasonable, but we identified a few occasions where officers did not sufficiently attempt to de-escalate.
There had been 17 uses of unfurnished accommodation in the last year. While they had all been appropriately authorised, accompanying paperwork did not always demonstrate sufficient justification.
Segregation
| HMIP prisoner survey | Yes | Compared with last inspection |
| Were you treated well by segregation staff? | 44% | Lower |
The segregation unit was busy and held some challenging individuals, some of whom had been there for very long periods. The average length of stay had more than doubled since our last inspection from 13 to 30 days.
The daily regime was affected by the number of prisoners on the unit and they were only able to shower every other day, which was unacceptable. The unit held a supply of books and prisoners could access distraction materials and in-cell education.
We observed some positive interactions between staff and prisoners on the unit, but day-to-day pressures limited opportunities for meaningful engagement.
Regular governance meetings had lapsed for more than five months and leaders were not analysing data or trends in segregation.
Despite this, individual reviews of segregated prisoners were thorough and multidisciplinary. We saw good examples of reintegration planning with involvement of the psychology team, and most men returned to the residential units.
The segregation unit was shabby and, in some places, bleak. Many cells on the lower floor needed refurbishment and exercise yards were austere.

Some prisoners on the main units had risk-based unlock arrangements, which required the presence of additional officers to open their cell doors. We were concerned that, in some cases, this was equivalent to segregation without the appropriate safeguards.
Security
Expected outcomes: Security and good order are maintained through an attention to physical and procedural matters, including effective security intelligence and positive staff-prisoner relationships. Prisoners are safe from exposure to substance misuse and effective drug supply reduction measures are in place.
| Data provided by the prison | |
| Positive random mandatory drug testing rate in the 12 months before the inspection | 9% |
In our survey, 56% of prisoners said that drugs were easy to get compared with 29% at our last inspection. Prisoners told us that drug use was driven by boredom, while leaders cited an increase in the complexity of the population, particularly in the level of those involved in organised crime.
Physical security measures were inadequate, including insecure windows, weak gate security and insufficient CCTV. Funding had been agreed by the long-term high security estate to address some of these weaknesses.
Those found to be using illicit substances were placed on the basic regime for 28 days and kept in their cells for 24 hours, which was punitive. A new drug strategy had a stronger focus on building recovery and offering support to those who used illicit substances, but there was still no incentivised substance free living unit (ISFL).
Security information was well managed. There was no backlog of intelligence reports and urgent information was responded to swiftly. Joint working with police and the local authority had improved, and more positive relationships had resulted in better organisation of work to combat drones.
A head of counter terrorism and corruption prevention had recently been appointed, and both extremism and corruption risks were well managed.
Safeguarding
Expected outcomes: The prison provides a safe environment which reduces the risk of self-harm and suicide. Prisoners at risk of self-harm or suicide are identified and given appropriate care and support. All vulnerable adults are identified, protected from harm and neglect and receive effective care and support.
Suicide and self-harm prevention
| Data provided by the prison | |
| Rate of incidents of self-harm per 1,000 prisoners in the 12 months before this inspection | 1,162 |
| Rate of incidents of self-harm per 1,000 prisoners in the 12 months before the last inspection | 1,614 |
There had been two self-inflicted deaths and one non-natural death since our last inspection. Recommendations made by the Prisons and Probation Ombudsman and local investigations were not regularly reviewed to check practice had improved. Not all incidents of serious self-harm had been fully investigated.
The rate of self-harm had reduced since our last inspection but was now increasing and the fifth highest of all adult male prisons. Leaders had used bespoke data to inform a new strategy, but their understanding of drivers remained limited. For example, ‘personal needs’ was cited as the main cause, but this covered a broad range of issues ranging from poor regime to unmet individual needs.
Reasons for self-harm were reviewed monthly but had yet to drive improvement; for example, behaviour management systems had been identified as a common trigger yet half of those supported by ACCT case management (Assessment, Care in Custody and Teamwork; the case management approach for prisoners at risk of suicide or self-harm) during our inspection were on the basic level of the incentives scheme.
Five highly complex prisoners, who accounted for nearly half of all self-harm incidents in the previous year, received good multidisciplinary support.
However, during the previous year, 124 individuals had self-harmed, which was a similar proportion to the last inspection. The range of support available for prisoners struggling to cope remained too limited, constrained further by the restrictive regime and staffing pressures. The community ethos on Houseblock 24 provided a supportive environment for those with a history of trauma (see Opportunities for prisoners to progress).
In our survey, only 51% of those supported by ACCT case management said they felt cared for by staff. Prisoners reported difficulties with accessing support from Listeners (prisoners trained by the Samaritans to provide emotional support to fellow prisoners).
There had been some improvements in the quality of ACCTs; for example, improved consistency of case managers. However, frailties remained; care plans too often did not address underlying issues, many case reviews were not multidisciplinary, and records did not always reflect meaningful engagement.
At the time of our inspection, one prisoner was subject to constant supervision. He was able to access the regime and was not unnecessarily restricted.
Protection of adults at risk
Leaders had recently established links with the local adult safeguarding board. Many staff lacked confidence in understanding safeguarding risks and there was no bespoke training to address this shortfall.
Section 3: Respect (Back to top)
Prisoners are treated with respect for their human dignity.
Staff/prisoner relationships
Expected outcomes: Prisoners are treated with respect by staff throughout their time in custody and are encouraged to take responsibility for their own actions and decisions.
In our survey of prisoners, 91% of prisoners aged 50 and over said that most staff treated them respect, compared to 73% of prisoners aged under 50.
We saw most staff engaging with prisoners in a friendly and confident manner. Prisoners were positive about staff and many identified individual members whom they found particularly helpful. However, relationships were often undermined by too many short-notice restrictions to the regime.
The frequency of key work (see Glossary) sessions had improved significantly (see Preparation for release).
The range and use of peer supporters had expanded since the last inspection, but some roles remained underdeveloped. While some peer workers, such as those on the trauma-informed unit, had received adequate training and oversight, others were not trained or supported (see Fair treatment and inclusion).
Daily life
Expected outcomes: Prisoners live in a clean and decent environment and are aware of the rules and routines of the prison. They are provided with essential basic services, are consulted regularly and can apply for additional services and assistance. The complaints and redress processes are efficient and fair.
Living conditions
| Data provided by the prison | |
| Proportion of the population living in overcrowded conditions at the time of the inspection | 17% |
Most cells were clean, free of graffiti and equipped to a reasonable standard. A work team of 12 prisoners supported maintenance across the prison, including minor repairs and replacing damaged flooring.
In Albany, most cells were very small and lacked a toilet and running water. An electronic night sanitation system allowed prisoners to join a queue for up to seven minutes to access the communal toilets. Prisoners could also request a portable camping toilet and a lidded bucket for use in their cells.
Many prisoners told us that they avoided using the electronic sanitation system. Although diluted disinfectant was provided to clean the portable toilets and buckets, both prisoners and staff reported that human waste was regularly thrown out of cell windows at night and landings smelt strongly of urine.
The areas immediately outside Albany were not routinely bio cleaned, and some sections remained contaminated with human waste. Grounds were otherwise well maintained, and outside exercise areas were spacious and included seating and exercise equipment.


Association equipment was in reasonable condition and new furniture had recently been added to many units. However, cleanliness in communal areas was inconsistent, with ingrained dirt on many landings and stairways.
Many showers were dirty, lacked privacy screens and had broken tiles. General oversight of decency and cleanliness was insufficient.


Access to prison clothing and bedding was reasonable. However, laundry facilities for personal clothing were poor, with many machines out of order and some prisoners waiting up to two weeks to wash their clothes. Replacement machines had been purchased and were awaiting installation.
Residential services
In our survey, 37% of prisoners said the food was good, similar to our last inspection. Around three-quarters of meals contained fresh produce and the portions and overall quality were good.
Serveries were clean, but supervision during mealtimes was inadequate. Some workers did not wear appropriate personal protective equipment and we saw meals being served with gloved hands rather than utensils. Meals were sometimes not served hot enough.
Across most wings, there was not enough opportunity to use self-catering facilities to support independent living, and prisoners had to eat in their cells.
Canteen provision included a good range of fresh and chilled produce. Over 200 items were ordered each week from a wide range of catalogues and an effective tracking database recorded each application from submission to delivery to the prisoner, providing good oversight of the process.
Prisoner consultation, applications and redress
Consultation with prisoners had improved. A prison council and ‘measuring the quality of prison life committee’ met leaders each month and wing managers held regular community meetings. This had resulted in meaningful changes which were regularly published.
The paper-based application system was managed very well; requests and responses were recorded and monitored on a database. Prison data showed that three-quarters of applications had been answered within seven days.
| Data provided by the prison | |
| Number of submitted complaints per 1,000 prisoners (March 2025 – February 2026) | 2,748 |
Complaints had reduced by about 12% since the last inspection. Most responses were polite and addressed the issues raised. However, there was no regular analysis of complaint data or actions taken to identify and address persistent concerns.
The library stocked relevant legal texts and there was adequate provision for legal face-to-face visits as well as video conferencing facilities for remote meetings.
Fair treatment and inclusion
Expected outcomes: There is a clear approach to promoting equality of opportunity, eliminating unlawful discrimination and fostering good relationships. The distinct needs of prisoners with particular protected characteristics (see Glossary) or those who may be at risk of discrimination or unequal treatment, are recognised and addressed. Prisoners are able to practise their religion. The chaplaincy plays a full part in prison life and contributes to prisoners’ overall care, support and rehabilitation.
Work to promote fair treatment had not been sufficiently prioritised. There was no strategy or needs analysis and action planning was underdeveloped. New leaders in this area had started to address these weaknesses and identify sensible and realistic short-term priorities.
Data had not been used well to drive improvement. Disproportionate outcomes had been identified in areas including the use of force on some minority ethnic and religious groups, but we did not see evidence that leaders had taken action to investigate or resolve this.
Consultation with most protected characteristic groups (see Glossary) was extremely limited and resulted in few actions to improve prisoners’ experiences. Forums were often cancelled because staff were not available and attendance at some was restricted to a small number of equality peer workers who did not necessarily represent the diversity of the population. The peer workers were motivated and demonstrated inclusive attitudes, but lacked sufficient training or oversight, a notable gap given their important advocacy role.
Complaints about discrimination were not always investigated thoroughly. Responses did not always address the substance of the complaint, and some were inappropriately redirected to the regular complaints process.
In our survey, prisoners from different groups reported similar experiences to their peers. Just under a quarter of the population were from minority ethnic groups. Those we spoke to did not highlight differences in treatment or discrimination, an improvement since the last inspection.
An inclusive range of purposeful activity, including wheelchair-accessible workshops, enabled those with low mobility to participate in the regime.
Support for neurodivergent prisoners was particularly good (see Mental health and Education, skills and work activities), with many supported by knowledgeable wing officers and a good range of purposeful and recreational activities.
Transgender prisoners told us they felt supported by most officers, although some reported disrespectful language from staff and prisoners. Those on the Parkhurst site were unable to attend the social coffee morning that was available on Albany, and the showers on their units did not afford sufficient privacy.
Faith and religion
Vacancies in the chaplaincy limited provision and there had not been a managing chaplain for over a year.
However, proactive and enthusiastic senior leadership had made sure that most faith groups were supported to some degree, including using volunteers and community organisations and facilitating peer-led groups and services.
Health, well-being and social care
Expected outcomes: Patients are cared for by services that assess and meet their health, social care and substance use needs and promote continuity of care on release. The standard of provision is similar to that which patients could expect to receive elsewhere in the community.
The inspection of health services was jointly undertaken by the Care Quality Commission (CQC) and HM Inspectorate of Prisons under a memorandum of understanding agreement between the agencies. The CQC found two breaches of regulations and issued requests for action plans following the inspection (see Appendix III).
Strategy, clinical governance and partnerships
In our survey, 57% of respondents considered the overall quality of health services to be very or quite good. Overall, we found that the quality and accessibility of health services were reasonable and most services had improved since our last inspection.
Practice Plus Group Health and Rehabilitation Services Limited (PPG) remained the primary health provider, with Time for Teeth delivering dental services, and Isle of Wight Council (IOWC) the local authority. All mental health and substance misuse services were now subcontracted to Midlands Partnership University NHS Foundation Trust (MPFT). NHS England monitored the contract through meetings and quality visits. A full health needs analysis and an impressive health inequality impact assessment had been completed in 2025.
The local health partnership had not given sufficient priority to addressing a range of longstanding issues affecting all health providers. These included the development of MPFT services and improvement of health facilities which did not meet infection prevention and control standards.
Some areas of governance were weak with insufficient managerial or clinical oversight, including incident management, clinical audit and complaints. Governance meetings did not demonstrate sufficient scrutiny of risks or quality and safety data. Oversight of safeguarding was good and there was a proactive approach to patient consultation.
SystmOne (electronic clinical records) was used across all services except social care and record-keeping standards were mostly good.
Emergency equipment and medicines were properly maintained and checked daily.
Promoting health and well-being
The delivery of the provider’s health promotion strategy was led by the Public Health Lead Nurse, supported by a small team. Health promotion started in reception and tests and vaccinations were offered during prisoners’ first two weeks. Monthly events were aligned with the NHS national calendar and some were advertised on in-cell televisions. Individualised health promotion also took place, including during discharge planning.
Meetings were held to hear patients’ views of services. Each wing had at least one prisoner health care representative. Sexual health services, including full STI screening, examinations and treatment, were available, and condoms could be confidentially requested.
Primary care and inpatient services
The primary care service operated every day with GP and advanced nurse practitioner sessions running throughout the week. Emergency nurse cover was always available with out-of-hours GP support. Most patients were seen promptly and a four-week wait for non-urgent GP appointments was an improvement.
Teamwork across health care was strong, enabling effective internal and external referrals. However, many external hospital appointments were cancelled through lack of prison staff and regime constraints. Daily handovers, weekday reviews of new arrivals and multidisciplinary meetings supported patients with complex needs.
The early days in custody team and the release and transfer nurse delivered a good service. Patients were contacted regularly during their first 14 days and good planning ensured safe transfer or release.
The position for a long-term conditions (LTC) nurse was vacant and the primary care team was delivering the service with senior clinical support. Most LTC care plans were not personalised and lacked key information which the primary care lead had started to address.
Patient records for ‘under the influence’ responses lacked important information, which increased risk.
End-of-life care was comprehensive, supported by a local hospice. The introduction of an on-site dialysis service was being explored to reduce the need for external hospital attendance.
The 18-bed inpatient unit was light and spacious. Patients had mental and/or physical health needs, but a few cells were often used for non-clinical admissions which could be disruptive for patients.
The unit was staffed by officers and physical health clinicians. Despite a high level of mental health need among patients, no staff had received mental health training. The mental health nurse post had been covered by a physical health nurse for an extended period and the mental health team was conducting daily patient assessments.
There were no therapeutic or constructive activities to maintain well-being and encourage recovery.
Social care
A draft Memorandum of Understanding and Service Level Agreement between PPG and IOWC was awaiting sign off from commissioners.
The robust referral process ensured prompt assessments and personalised care plans were delivered by IOWC. However, documentation was on paper and not on SystmOne, which created a risk. Seven prisoners were receiving care packages. Carers were well trained and delivered an excellent, responsive service that was highly valued by those receiving support.
Risk-assessed peer support workers helped with domestic tasks, although not all had received formal training. Those we spoke to had job descriptions and understood their roles. Equipment to support independence was available, but some prisoners experienced long waits for it.
Mental health
The team operated seven days a week and supported 136 patients (around 14% of the population), in addition to those seen only by the psychiatrist. Despite improved staffing, there were vacancies for a psychologist and learning disability nurse and the psychiatrist and mental health nurses supported neurodivergent patients. Newly appointed staff were not yet fully operational and the service was prioritising patients in crisis and those assessed as highest risk or lowest need. This reduced support for individuals with moderate needs.
The team received around 50 referrals each month. Outcomes were reviewed at daily meetings with the substance misuse service and patients allocated to appropriate pathways. Prison staff described the team as responsive to urgent issues, but not always available to review patients on the wings.
Patients with mild to moderate needs were offered evidence-based one-to-one interventions, self-help resources and limited groups. Eye movement desensitisation reprocessing therapy was available, but there were no high intensity groups. Patients spoke positively about their care but wanted more frequent appointments.
The full-time psychiatrist delivered four on-site sessions a week and a monthly MMPSA clinic (see Glossary) and was available for clinical advice. Care planning, risk management and physical health monitoring were effective, and aftercare on transfer or release was well managed.
Five patients had been accepted for transfer to secure services under the Mental Health Act in the past year, four of whom waited longer than the national guideline, which was poor.
Support and treatment for prisoners with addictions and those who misuse substances
Substance misuse services were reasonably well integrated into the prison’s drug strategy agenda. In our survey, 13% of respondents reported a drug or alcohol problem.
The clinical team had no vacancies and provided a seven-day service. New arrivals were seen promptly and treatment was continued or started when clinically indicated. Patients requiring observation were admitted to the inpatient unit. Treatment reviews were rarely attended by the psychosocial team and patients did not receive personalised care plans, which was poor. At the time of the inspection, 47 patients were receiving opiate substitution therapy, but treatment options were limited because eligibility for long-acting buprenorphine injections was based on sentence length rather than clinical need. Non-medical prescribers worked closely with GP and mental health prescribers to support patients.
The psychosocial team had experienced staff shortages and the service had yet to function effectively. The team supported 120 clients with high intensity needs and 35 with low intensity needs. The team had supported 26 patients identified as under the influence of illicit substances in the first two months of the year. However, there was no coordinated approach to supporting patients who were frequent users of illicit substances.
Referrals from various sources were assessed promptly, but too few one-to-one and group interventions were delivered across both sites. Only Albany had peer recovery champions, and mutual aid (including Alcoholics Anonymous) was delivered only on alternate months at each site.
Prison staff had not received substance misuse awareness training, but they were trained in the use of nasal naloxone to treat opiate overdose. Release planning was managed effectively, with staff notifying community drug teams and arranging prescriptions.
Medicines optimisation and pharmacy services
Medicines management processes had improved since our last inspection. The on-site pharmacy dispensed medicines safely and promptly, with out-of-hours access supported by suitable audit trails. Two full-time pharmacists clinically screened prescriptions, although they did not deliver clinics or undertake medication reviews, which limited opportunities to strengthen patient care. A range of patient group directives (to enable nurses to supply and administer prescription-only medicines) and a clear homely remedies policy enabled the safe supply of additional medicines.
Administration of not in-possession medicines was carried out three times a day by pharmacy technicians and nurses. Supervision by officers remained inconsistent, increasing the risk of concealment. Medicines were labelled and stored in line with legal and professional requirements. SystmOne was used effectively to document prescribing, administration and non-attendance. Patients who missed critical medicines were followed up promptly.
Around 70% of patients received medicines in possession (IP). Risk assessments were completed and reviewed at least annually, with compliance packs provided where needed. Random cell checks were undertaken and non-compliance led to reconsideration of IP status. Medicines were accessible when the pharmacy was closed and stock was stored appropriately.
Medication errors were addressed effectively. Advance notice of releases, transfers and court appearances enabled timely preparation of medicines. Transport arrangements, including for high-risk items, were appropriate. Drug safety alerts were actioned correctly and both confidential and medicines waste were disposed of in line with regulations.
Dental services and oral health
Time for Teeth delivered seven dentist and two therapist sessions every week.
At the time of our inspection, the waiting time was around five weeks, although those experiencing facial swelling or severe dental pain could be seen at the next session.
Dental care records were detailed and indicated that patients received appropriate assessment, treatment and oral health instruction.
Governance was strong and key areas of safety such as radiography, infection control, invasive procedures and dental unit waterlines were managed well. Records showed that dental equipment had been maintained and serviced to ensure it was safe for use. However, dental surgeries were shabby, cramped and cluttered.

Section 4: Purposeful activity (Back to top)
Prisoners are able and expected to engage in activity that is likely to benefit them.
Time out of cell
Expected outcomes: All prisoners have sufficient time out of cell (see Glossary) and are encouraged to engage in recreational and social activities which support their well-being and promote effective rehabilitation.
| HMIP prisoner survey | Yes | Compared with last inspection |
| Do you usually spend less than two hours out of your cell each day on Monday–Friday? | 20% | No difference |
Prisoners spent too much time in their cells. In our roll checks, we found about one-third of prisoners locked up during the working day, which was far too many for a training prison. While those working full time could spend around 8.25 hours a day unlocked during the week, for many prisoners this could be as little as 2.5 hours. These included the retired, sick and others who could not attend work, for example due to workshop closures.
An increase in the number of prisoners deemed ‘high risk’ contributed to the shortage of suitable full-time purposeful activity spaces. Some prisoners were left without a job and others had been moved from full-time into part-time work, reducing the time unlocked.
Association was not available during the week, except on Friday afternoons for enhanced prisoners, and the regime at weekends was poor.
PE facilities were good. The gym timetable continued to offer an impressive range of activities each day to meet the needs and preferences of the diverse population. This included team sports, Park Run, fitness challenges, darts, dominoes and hobby/card games.
Libraries were well run and offered a good service. There was a larger and more relevant selection of books in languages other than English than we usually see, and some good initiatives to promote reading for pleasure. There were dedicated sessions for neurodivergent prisoners and for legal study (see Fair treatment and inclusion and Education, skills and work activities).
Education, skills and work activities
Ofsted inspects the provision of education, skills and work in custodial establishments in England. The following summary has been provided by Ofsted inspectors who attended this inspection. Their full report is published under ‘Further resources’.
Ofsted made the following assessments about the education, skills and work provision:
- Overall effectiveness: requires improvement
- Quality of education: requires improvement
- Behaviour and attitudes: requires improvement
- Personal development: requires improvement
- Leadership and management: requires improvement
Leaders had taken action to address the concerns identified at the previous inspection, including improving aspects of the curriculum and quality assurance.
Leaders did not ensure prisoners engaged in sufficient purposeful activity. Leaders had not ensured the prisoners were allocated to sufficient part-time education, skills and work to enable consistent participation and effective use of their time. Many prisoners attended part-time activities or their time was split across multiple activities, which limited the continuity of their studies and reduced the impact on their progress. Although most prisoners had an allocated activity, leaders did not have an adequately accurate understanding of the proportion of prisoners engaged in full-time or part-time activities or those undertaking multiple activities.
Leaders had developed a broad curriculum that included education, vocational training and higher-level opportunities, with intended pathways to support progression to employment. However, implementation was not consistently effective. Some prisoners did not access well-planned coherent programmes that enabled them to build their knowledge and skills over time.
Leaders monitored attendance and followed up absence. Prisoners who attended activities arrived punctually and ready to start their activity. However, their actions had not secured consistently high attendance and participation in education.
The education provider, Milton Keynes College, ensured that staff were appropriately qualified. In the stronger subjects, teachers used questioning, assessment and resources appropriately to support learning. Peer mentors supported prisoners’ engagement and confidence. The inconsistent use of starting points limited how well teaching met prisoners’ needs; this meant that some prisoners completed work that was too easy while others struggled to keep up.
Prisoners developed practical skills in vocational areas and took pride in their work. However, work activities did not consistently focus on developing relevant knowledge, skills and behaviours or lead to meaningful accreditation. Leaders had not ensured that prisoners’ progress in workshops was monitored effectively, limiting their ability to identify gaps in learning or support progression.
Most prisoners who completed their courses achieved their qualifications, although achievement in mathematics was weaker. Too many prisoners did not sustain their learning or complete their courses. Leaders’ analysis of participation, withdrawals and outcomes was not sufficiently developed to identify patterns or take timely action to improve retention and achievement.
Support for prisoners with neurodiverse needs was effective. Staff identified needs and provided appropriate support, enabling most prisoners to engage and make progress. Prisoners valued the support they received and were able to access learning with increased confidence.
Careers information, advice and guidance were in place but were not sufficiently timely or comprehensive. Backlogs remained, limiting how well some prisoners were supported to make informed decisions about their next steps.
Leaders had established a well-considered reading strategy, supported by appropriate library provision and effective peer support. Most prisoners benefited from opportunities to develop their reading skills and engaged positively with reading. Targeted support enabled prisoners with lower starting points to improve their confidence and ability.
Although leaders had developed thoughtful, prisoner-informed plans, personal development remained underdeveloped. The curriculum lacked coherence, enrichment was limited, and leaders did not monitor participation or impact. As a result, many prisoners did not gain the wider knowledge, skills and behaviours needed for progression and release.
Section 5: Preparation for release (Back to top)
Preparation for release is understood as a core function of the prison. Prisoners are supported to maintain and develop relationships with their family and friends. Prisoners are helped to reduce their likelihood of reoffending and their risk of harm is managed effectively. Prisoners are prepared for their release back into the community.
Children and families and contact with the outside world
Expected outcomes: The prison understands the importance of family ties to resettlement and reducing the risk of reoffending. The prison promotes and supports prisoners’ contact with their families and friends. Programmes aimed at developing parenting and relationship skills are facilitated by the prison. Prisoners not receiving visits are supported in other ways to establish or maintain family support.
Many prisoners’ families faced long journeys and high ferry costs. On arrival, the visitors’ centre provided refreshments, activities for children and a comfortable place to wait.

Visits took place on Friday, Saturday and Sunday afternoons, but the two-hour sessions could not be extended for prisoners whose families travelled long distances. Visits areas were equipped with a good range of toys and games.


Local monitoring indicated that only 250 prisoners had received a visit in the previous 12 months, but data were not collected on those who had never received a visit. This made it difficult to support those who were most isolated.
Video calls provision was particularly good, with sessions available every day. Over the previous 12 months, 33% of prisoners had made nearly 10,000 calls.
Barnardo’s, the family services provider, delivered monthly family days (see Glossary) in both sites and facilitated a monthly fathers’ peer support forum. They also ran the Storybook Dads scheme (in which prisoners record stories to send to their children) and provided a homework club during visits. There were still no parenting courses available, but staff had recently been trained by The Centre for Emotional Health to deliver a nurturing course.
Quarterly visitor forums were held by leaders, both in person and online, which helped to improve the overall visitor experience.
Reducing reoffending
Expected outcomes: Prisoners are helped to change behaviours that contribute to offending. Staff help prisoners to demonstrate their progress.
| Data provided by the prison | |
| Highest probation POM caseload at the time of the inspection | 121 |
The population profile had changed since the last inspection, and the prison was now evenly split between category B and C PCOSOs, with a small remand population. Over 85% presented a high risk of harm.
A reducing reoffending strategy was now in place and the needs analysis supporting the strategy had included prisoners’ comments. Meetings to support delivery of the strategy were appropriately attended and the sense of direction in the prison was clearer.
Leadership in the offender management unit (OMU) had improved since our previous inspection. However, intractable challenges in recruiting prison offender managers (POMs) continued to affect prisoners.
There was also a shortfall in senior probation officers (SPOs). One of the SPOs in place at the time of our last inspection remained in post, providing continuity, focus and leadership. More recently, this SPO had been supported by a colleague working remotely.
How staff were supporting prisoners and managing risk
Prisoners were appropriately allocated a probation POM, but unmanageable caseloads limited meaningful one-to-one work.
Leaders had maximised prisoner contact by bringing trainee probation staff and probation service officers (PSOs) into the OMU. Together with the prison POMs, they provided day-to-day contact with prisoners, enhanced by regular OMU surgeries. An external probation officer provided support by writing OASys reports remotely.
Prisoners were well supported by good key work delivered each month. There was evidence of these sessions being informed by sentence plan targets. However, key workers often changed when prisoners moved wings, and quality assurance checks by managers were not always reliable.
Over 80% of prisoners knew their sentence plan targets and most of the prisoners we met could name someone who was supporting them to make progress. This was often a supporting POM, psychologist, key worker or wing officer.
There were 37 IPP prisoners (imprisonment for public protection sentences.) at the time of the inspection, with 10 having progressed out of the prison in the last year, who received good support. Strong links between the OMU and psychology were supported by prison-wide review meetings.
Prisoners whose level of risk required their communications to be monitored were identified efficiently and checks were reasonably up to date. Authorisations for monitoring were not always timely, resulting in some cases in gaps in monitoring after an earlier authority had lapsed.
Opportunities for prisoners to progress
While there were good opportunities for prisoners to progress and reduce their risk, these were available only to a limited number of men.
An experienced and flexible programmes team were delivering all strands of the new accredited programme, including to those with learning difficulties. However, there was a high attrition rate of over a third for the prisoners in the high risk, high need groups completing this programme, which was concerning.

Some prisoners completed a foundation course to prepare them to take part in programmes, and a very small number of the most complex PCOSOs completed the healthy sex programme.
The dedicated unit for prisoners with a history of trauma provided an effective community to help men to understand and address offending behaviours, despite limited resources. The timetable included a good range of group work to increase understanding of how trauma affects the body and to build knowledge of risk management and the probation service. Prisoners said that being part of the unit had helped them change their lives.
Prisoners were involved in the recategorisation process, although 72% of reviews in the last 12 months had been completed late. Transfers for category C prisoners were often delayed, which created a barrier to progression for many.
Returning to the community
Expected outcomes: Prisoners’ specific reintegration needs are met through good multi-agency working to maximise the likelihood of successful resettlement on release.
| HMIP prisoner survey | Yes | Compared with similar prisons |
| For those who expect to be released in the next three months, do you need help with getting photo ID for when you are released? | 94% | Higher |
| Are you getting help to sort out getting photo ID for when you are released, if you need it? | 13% | Lower |
Prison leaders had been pragmatic in the use of resources to meet the resettlement needs of the population.
Since the last inspection, the number of prisoners being released had increased, most of whom were serving short sentences or on remand. The needs of these prisoners were identified on arrival by a pre-release officer and were discussed at regular multidisciplinary meetings where staff planned for likely court outcomes. These meetings were regularly attended by the local homelessness prevention lead and a DWP work coach. However, remanded prisoners did not receive support to obtain photo ID, which was a gap.
Of the 133 releases in the last 12 months, prison data showed that 8% were homeless on their first night. However, data were only recorded for those under probation supervision, meaning the true figure was likely to be higher.
Almost all long-term prisoners were transferred to a more suitable establishment before release. However, this often happened too close to the release date, which reduced the time available for practical resettlement support.

Most prisoners within three years of their release date lived on the resettlement unit. Those due for release within 18 months or with approaching parole reviews were able to complete a resettlement course which covered budgeting, staying safe online, coping strategies, and developing a CV and disclosure letter.

The release plans of all high-risk prisoners were reviewed by a regular and well-attended interdepartmental risk management meeting. We saw evidence of effective escalation to obtain last-minute housing where Approved Premise places had been withdrawn, or release dates had changed.
However, we found some prisoners due for release in less than six months who had not had their MAPPA levels (see Glossary) confirmed. Written contributions to community public protection meetings were good and attendance was appropriate.
There was no departure lounge and support on the day of release was limited.
Section 6: About HMP Isle of Wight (Back to top)
Category of the prison
A designated category B male training prison, predominantly for prisoners convicted of sexual offences with a small local remand function
Brief history
HMP Isle of Wight was formed in 2009 through the merger of three historic prisons: Parkhurst (opened 1838), Albany (established as a prison in 1967), and Camp Hill (1912). Camp Hill later closed in 2013, leaving Parkhurst and Albany continuing as the two operational sites.
Population
Prisoners held at the time of inspection: 961
Baseline certified normal capacity: 931
In-use certified normal capacity: 879
Operational capacity: 968 (reduced by 131 for fire safety improvement work)
- 367 new prisoners received each year
- 95 foreign national prisoners
- 23% of prisoners from black and minority ethnic backgrounds
- 62 prisoners released into the community in the past year
- 146 prisoners receiving support from SMS
- 650 prisoners referred for mental health assessment in the past year
Short description of residential units
HMP Isle of Wight consists of two separate sites separated by a road.
Albany site
The Albany site contains seven housing units and a specialist healthcare unit.
HB10: inpatient healthcare unit
HB11: induction unit.
HB12–HB15: PCOSO population.
HB16: remand unit.
HB17: PCOSO population
Parkhurst site
The Parkhurst site contains seven housing units and a separate segregation unit.
HB18: currently not in use
HB19: currently under refurbishment
HB20–HB22: PCOSO population
HB23: enhanced unit
HB24: therapeutic ‘trauma-informed’ support unit
HB25: segregation unit
Prison status (public/private)
Public
Key providers
Physical health provider: Practice Plus Group (PPG)
Mental health provider: Midlands Partnership Foundation Trust
Substance misuse treatment provider: Midlands Partnership Foundation Trust
Dental health provider: Time for Teeth
Prison education framework provider: Milton Keynes College
Escort contractor: Serco
Prison group director
Hannah Lane, long-term and high security group South
Name of governor/director and date in post
Dougie Graham, May 2018 –
Independent Monitoring Board Chair
Christine Dyson
Date of last inspection
20 September – 7 October 2022
Progress on concerns from the last inspection (Back to top)
At our last inspection in 2022 we raised 15 concerns, six of which were about areas of priority concern.
At this inspection we found the following progress:
The following is a list of all the concerns raised, organised under the four tests of a healthy prison.
Leadership
Key concerns
Data were not used well enough to improve outcomes. Managers did not explore outcomes at other prisons holding a similar population, including those convicted of sexual offences and category C prisoners. They did not evaluate the impact of the education and skills curriculum to drive improvement.
Not addressed
Over a third of officers were not available for work in the units, which limited the delivery of the day-to-day regime and led to prisoners spending too long locked in cells.
Not addressed
Safety
Priority concern
The health provider had identified risks to service delivery and patient outcomes, but improvements had not taken place quickly enough.
Not addressed
Key concerns
Many of the residential units were shabby, bleak and in need of significant repair.
Partially addressed
Black and minority ethnic and Muslim prisoners and those with mental health problems were far more negative than their counterparts about some key aspects of their care, for example, their relationships with staff and the safety outcomes they experienced.
Addressed
Mental health and learning disability services did not provide adequate or timely evidence-based care or treatment.
Not addressed
There was insufficient oversight of, and control over, medicines creating risks to staff and patients.
Addressed
Purposeful activity
Priority concern
Prisoners had very limited access to work or study. Planned access was severely undermined by poor attendance, poor punctuality and prisoners returning to their cells early.
Addressed
Key concerns
Leaders had not prioritised reading or literacy.
Addressed
Leaders did not make sure that prisoners could access education promptly enough to make progress towards their career aspirations.
Addressed
Preparation for release/Rehabilitation and release planning
Priority concerns
The therapeutic and rehabilitative purpose of the prison was not sufficiently prioritised. Leaders had not developed the environment or regime in a way that sought to ensure needs and risks of the sex offender population were addressed. This was compounded by a failure to respond to the new reality of a much larger population of category C prisoners. Specialist staff shortages further worsened this situation.
Not addressed
There were significant gaps in release planning for prisoners, many of whom posed a high risk of serious harm to the public.
Addressed
Key concerns
Prison offender managers did not have enough contact with prisoners or access to interventions to help them address their offending behaviour.
Not addressed
There was too little support to help prisoners maintain or rebuild ties with their families and friends and no reliable resettlement help for those being released.
Addressed
Care Quality Commission Action Plan (Back to top)
Care Quality Commission (CQC) is the independent regulator of health and adult social care in England. It monitors, inspects and regulates services to make sure they meet fundamental standards of quality and safety. For information on CQC’s standards of care and the action it takes to improve services, please visit: http://www.cqc.org.uk
The inspection of health services at HMP Isle of Wight was jointly undertaken by the CQC and HMI Prisons under a memorandum of understanding agreement between the agencies (see Working with partners) for action plans following this inspection. The Care Quality Commission issued a request for an action plan following this inspection.
Action Plan Request
Provider
Practice Plus Group Health and Rehabilitation Services Limited
Location
HMP Isle of Wight
Location ID
1-4969609615
Regulated activities
Diagnostic and screening procedures and treatment of disease, disorder or injury.
Action we have told the provider to take
This notice shows the regulations that were not being met. The provider must send CQC a report describing what action it is going to take to meet these regulations.
Regulation 17 – Good governance
How the regulation was not being met:
- Meeting minutes including those for, the Local Delivery Board, Quality Assurance Meetings, Patient Safety Meetings and Medicines Management, did not contain sufficient evidence or detail of scrutiny around quality and safety.
- PPG did not have adequate oversight of the performance and service delivery of the sub-contracted inclusion service. This meant the inclusion service was not well integrated within the healthcare team.
- The risk register did not capture all risks and there was no evidence that the risk register had been reviewed at key meetings with partners.
- There was poor oversight of the incident reporting processes. There were several investigations outstanding, some dating back to October 2025.
- The patient complaint leaflet was not available on all wings and there was not adequate guidance to support patients to make a complaint. Complaints were separated into categories of complaints or concerns and frequently there was no distinction or rationale between these categories.
- There was insufficient oversight to ensure action plans from audits were time specific, implemented and closed.
- Patient records, specifically, emergency responses to “Under the Influence” emergencies and long-term condition and substance misuse care plans lacked relevant information to help ensure patients received safe care.
Regulation 18 – Staffing
How the regulation was not being met:
- Staff working on the inpatient unit did not have the required skills to ensure patients with mental health needs received the required level of care and intervention.
- The psychologist position was vacant which limited the therapeutic interventions available to patients.
More about this report (Back to top)
This report outlines the priority and key concerns from the inspection and our judgements against the four healthy prison tests. Each of the following four sections contains a detailed account of our findings against our Expectations for men’s prisons.
Find out more about our Expectations and how we inspect
Find out more about priority and key concerns
Find out about notable positive practice
Findings from the survey of prisoners and a detailed description of the survey methodology are published alongside this report. Please note that we only refer to comparisons with other comparable establishments or previous inspections when these are statistically significant. The significance level is set at 0.01, which means that there is only a 1% chance that the difference in results is due to chance.
The tables in this report which provide data from HMI Prisons prisoner surveys also include comparisons with similar prisons.
| Description | What it means |
| Lower | the prison’s percentage is statistically significantly lower than the comparator: prisons with the same function type, or at the last inspection |
| Higher | the prison’s percentage is statistically significantly higher than the comparator: prisons with the same function type, or at the last inspection |
| No difference | the prison’s percentage is not statistically significantly different to the comparator: prisons with the same function type, or at the last inspection |
Inspection team
This inspection was carried out by:
Charlie Taylor, Chief inspector
Sara Pennington, Team leader
Harriet Leaver, Inspector
Rick Wright, Inspector
Jessie Wilson, Inspector
Dawn Mauldon, Inspector
Lindsay Jones, Inspector
Tareek Deacon, Researcher
Sophie Riley, Researcher
Joe Simmonds, Researcher
Emma King, Researcher
Samantha Moses, Researcher
Simon Newman, Lead health and social care inspector
Lynn Glassup, Health and social care inspector
Angela Star, Health and social care inspector
Lindsay Woodford, General Pharmaceutical Council inspector
Bev Gray, Care Quality Commission inspector
Carolyn Brownsea, Ofsted inspector
Diane Koppitt Ofsted inspector
Sarah Alexander, Ofsted inspector
Martyn Griffiths, Offender management inspector
Find out more about the terms and abbreviations used in this report in our glossary.
Easy read summary and press notice (Back to top)
Survey materials and Ofsted full report (Back to top)
The following files may not be suitable for users of assistive technology.
Request an accessible format
If you use assistive technology (such as a screen reader) and need a version of any of these documents in a more accessible format, please email media@hmiprisons.gov.uk. Please tell us what format you need. It will help us if you say what assistive technology you use.