
HMP Aylesbury
Report on an unannounced inspection of HMP Aylesbury by HM Chief Inspector of Prisons 2–12 February 2026

Introduction (Back to top)
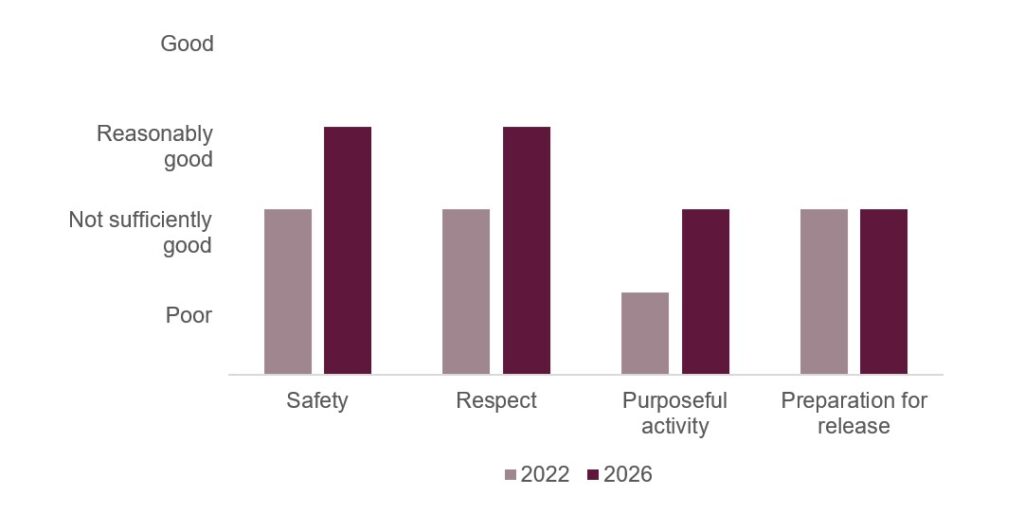
Aylesbury is a category C training prison, which at the time of this inspection was holding up to 370 adult men. Largely built during the 19th century, the prison was not without its challenges, but thanks to some committed leadership and staff professionalism, this inspection found a prison that evidenced some significant improvements. We last inspected in 2022, when the prison was adjusting to a new designation and role, having previously held long-term young adults. At that time, outcomes in three of the healthy prison tests were judged to be ‘insufficient’, and purposeful activity was ‘poor’. During this inspection, outcomes in safety and respect had clearly improved and were now ‘reasonably good’. In purposeful activity and preparation for release, however, much remained to do, although the provision of both was clearly improving.
The prison was much safer, with levels of violence lower than in comparable institutions. Staff knew their population well and were generally proactive in identifying risks, particularly for those newly arrived, or at risk of self-harm. Arrangements to support vulnerable prisoners were in place and used appropriately. The prison was stable and most prisoners felt safe and encouraged to behave well. However, this did not translate into positive well-being for all. There had been a significant upturn in self-harm incidents and, although formal arrangements were in place to support those at risk, ACCT processes were not robust, with weaknesses in case coordination and care planning. Substance misuse also remained a key challenge, with data indicating that around a quarter of the population were active drug users.
Relationships between staff and prisoners were positive. Staff treated prisoners with respect and were confident in managing behaviour. Leaders maintained a clear focus on decency, and living conditions were generally reasonable. Although parts of the ageing estate undermined the overall environment, access to basic services was mostly adequate and the prison was clean. All prisoners had their own cell and, overall, living conditions were good.
Purposeful activity was improving, supported by good time out of cell and low unemployment, and leaders had begun to strengthen employer engagement through an Employment Advisory Board. However, the quality and impact of education, training and work were not yet sufficient. Curriculum breadth was limited, attendance was inconsistent, and too many prisoners did not benefit from activity that was sufficiently demanding or purposeful.
Preparation for release required further development. Despite some promising initiatives and specialist provision for small cohorts, offender management and progression were inconsistent and not always timely. Sentence plans were not consistently kept up to date, contact for many prisoners was limited, and delays in accessing accredited programmes hindered progress.
Overall, HMP Aylesbury is an improving prison that has benefited from committed staff and a clear sense of purpose from senior leaders. The priority now is to consolidate and embed delivery, particularly in relation to drugs, self-harm processes, education and offender management, to ensure that ambition translates reliably into further improvements in outcomes for prisoners.
Charlie Taylor, HM Chief Inspector of Prisons, March 2026
Outcomes for prisoners (Back to top)
We assess outcomes for prisoners against four healthy prison tests: safety, respect, purposeful activity, and preparation for release (see More about this report for more information about the tests). We also include a commentary on leadership in the prison (see Section 1).
At this inspection of HMP Aylesbury, we found that outcomes for prisoners were:
- Reasonably good for safety
- Reasonably good for respect
- Not sufficiently good for purposeful activity
- Not sufficiently good for preparation for release.
We last inspected Aylesbury in 2022. Figure 1 shows how outcomes for prisoners have changed since the last inspection.
Figure 1: Aylesbury healthy prison outcomes 2022 and 2026
What needs to improve (Back to top)
During this inspection we identified 10 key concerns, of which four should be treated as priorities. Priority concerns are those that are most important to improving outcomes for prisoners. They require immediate attention by leaders and managers.
| Priority concerns | |
| 1. | Illicit drug use was high and undermined safety. |
| 2. | Rates of self‑harm were high and increasing. ACCT processes were not consistently robust, with inconsistent case coordination, sparse care plans and gaps in record‑keeping. |
| 3. | Leaders had not implemented a sufficiently broad or ambitious curriculum that met the needs or interests of all prisoners. |
| 4. | Many prisoners waited too long for an initial sentence progression plan, and offender management support was inconsistent and too often delayed. This limited prisoners’ ability to progress through their sentence. |
| Key concerns | |
| 5. | Key work was not yet consistent or embedded. |
| 6. | The applications system was ineffective. Prisoners often did not receive responses and there was no effective tracking or oversight. |
| 7. | There were insufficient prison escorts to meet the clinical needs of the population. This created shortfalls in access to care and treatment, which created unnecessary clinical risk. |
| 8. | Leaders had not made sure that all work was sufficiently demanding or purposeful for prisoners. Too many prisoners did not value their work roles. |
| 9. | Too many prisoners did not attend the education, skills and work provision. |
| 10. | Teaching staff did not consistently revisit prisoners’ learning on radicalisation and extremism. Most prisoners engaged in education did not understand the associated risks. |
Notable positive practice (Back to top)
We define notable positive practice as evidence of our expectations being met to deliver particularly good outcomes for prisoners, and/or particularly original or creative approaches to problem solving. Inspectors found four examples of notable positive practice during this inspection, which other prisons may be able to learn from or replicate.
| 1. | A use of force staff training package had been developed that supported staff understanding of use of force scrutiny processes. (See Use of force) |
| 2. | The weekly review and response meeting offered effective oversight and support for prisoners reported to be under the influence of illicit drugs. (See Security) |
| 3. | The incentivised substance free living unit (ISFL) was a more effective and better‑developed model than we usually see. Strong staff and peer support fostered a sense of community, and the on‑wing presence of substance misuse services, improved facilities and increased time out of cell provided meaningful incentives for prisoners to remain substance free. (See Security, Living Conditions, Support and treatment for prisoners with addictions and those who misuse substances and Time out of cell) |
| 4. | An impressive accessibility visits room offered a private and calm environment for vulnerable visitors. (See Children and families and contact with the outside world) |
Unless otherwise specified, these examples are not formally evaluated, are a snapshot in time and may not be suitable for other establishments. They show some of the ways our expectations might be met, but are by no means the only way.
Section 1: Leadership (Back to top)
Leaders provide the direction, encouragement and resources to enable good outcomes for prisoners.
The governor had been in post for just over 18 months and had set a clear sense of direction for the prison, supported by improved communication and a four-year strategy recognised by staff and prisoners. Recruitment and retention had strengthened since the previous inspection, which had improved staffing stability and underpinned more consistent delivery.
Leaders used consultation with staff, prisoners and partners to shape priorities and create a more engaged working environment. This approach produced visible changes, including the Academy wing for those involved in learning, an impressive incentivised substance-free living (ISFL) unit (see Glossary), alongside new provision for prisoners serving indeterminate sentences. These developments reflected ambition; however, several were at an early stage and not yet embedded in everyday practice.
Assurance was mixed and although there was a sense of confidence in the prison leadership, some information shared with us in advance did not match what we found on site, and data were not always used well enough to identify and address emerging safety risks. Governance had contributed to a reduction in violence, but leaders were not sufficiently focused on the widespread availability of illicit substances or the rising level of self-harm, both of which continued to place pressure on the prison. Decency was broadly maintained through local effort, but limited investment from HM Prison and Probation Service (HMPPS) in updating closed-circuit television equipment hindered work to disrupt the ingress of illicit items effectively.
Leaders took a determined approach to rebuilding purposeful activity and strengthening links with employers, but the quality and consistency of education, skills and work, particularly curriculum breadth, planning and attendance, were below the standard expected in a training prison. Health care leadership, including for substance misuse, had improved, with more stable staffing and effective partnership working. However, key aspects of offender management were not delivered consistently or early enough for all prisoners.
Section 2: Safety (Back to top)
Prisoners, particularly the most vulnerable, are held safely.
Early days in custody
Expected outcomes: Prisoners transferring to and from the prison are safe and treated decently. On arrival prisoners are safe and treated with respect. Risks are identified and addressed at reception. Prisoners are supported on their first night. Induction is comprehensive.
| HMIP prisoner survey | Yes | Compared with similar prisons |
| When you arrived at this prison, did you spend less than 2 hours in reception? | 59% | Higher |
| HMIP prisoner survey | Yes | Compared with last inspection |
| Overall, were you treated very/quite well in reception? | 87% | Higher |
Early days arrangements had improved. Around eight prisoners arrived each week, many from out of area. The bright, spacious reception facility, along with swift processes and good support from induction staff and peer advisers, helped settle prisoners quickly.

New arrivals were searched and property was issued without delay. The X‑ray body scanner was used subject to risk assessment, but not as frequently as we would expect, given the ongoing concerns about the ingress of illicit items (see also Security).
An initial first night risk interview was completed in reception and identified immediate safety concerns. However, it was not conducted in private, which meant that sensitive information could be overheard. Follow‑up support interviews during the two‑week induction period were held confidentially.

| HMIP prisoner survey | Yes | Compared with similar prisons |
| Did you feel safe on your first night here? | 90% | Higher |
The first night centre was clean, and cells were well prepared. Prisoners were offered grocery packs and showers and were able to contact family or friends before being locked up. Additional welfare checks were completed routinely during the first night.

Induction was delivered by staff and prisoner peer advisers. A welcome booklet contained appropriate information about what to expect and a weekly induction fair introduced prisoners promptly to other departments that could support their early needs, such as offender management and substance misuse services.

Oversight of induction was good, and managers made sure that most new arrivals completed induction before moving to other wings. In our survey, 93% of respondents said that they had received an induction.
Promoting positive behaviour
Expected outcomes: Prisoners live in a safe, well ordered and motivational environment where their positive behaviour is promoted and rewarded. Unacceptable conduct is dealt with in an objective, fair, proportionate and consistent manner.
Encouraging positive behaviour
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Do you think the culture within this prison encourages prisoners to behave well? | 34% | Higher |
Many prisoners told us that the predictable regime, clear communication, sufficient time out of cell and the development of specialist units, including the ISFL unit and Academy wing, encouraged positive behaviour. This was reflected in improved perceptions of safety since the previous inspection and a sharp reduction in the number of violent incidents, which was lower than in similar prisons, with few serious assaults.
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Have you ever felt unsafe here? | 27% | Lower |
The safety team was well resourced and there was effective information sharing between safety and security departments. Intelligence for all new arrivals was reviewed, and conflicts or concerns were addressed appropriately during induction interviews.
Challenge, support and intervention plan (see Glossary) investigations were completed in all relevant cases, used effectively for fact finding and generally of good quality, leading to appropriate referrals. However, when support plans were opened, they often lacked detail and did not fully make use of the available interventions.
Joint monthly meetings between the safety, security and drug strategy teams provided a reasonable forum for sharing information and responding to immediate concerns. However, these meetings were underdeveloped and did not make enough use of the available data.
The most common adjudication charges were for unauthorised items, including illicit drugs, reflecting the wider security challenges that leaders faced (see also Security). While oversight had improved, some hearings still lacked sufficient enquiry.
Use of force
| Data provided by the prison | |
| Rate of recorded use of force incidents per 1,000 prisoners in the 12 months prior to the inspection | 721 |
Use of force had reduced steadily since the previous inspection and was now broadly in line with that at similar category C prisons. High‑level interventions were rare, with no employment of PAVA spray (see Glossary), two baton strikes and three uses of unfurnished accommodation.
The use of body‑worn cameras had improved significantly, with footage available for 88% of incidents. Staff reported occasional difficulties in accessing cameras, which resulted in a few incidents not being recorded, but leaders were taking action to address this.
The use of force coordinator debriefed most prisoners following incidents and had introduced a training package that clarified scrutiny arrangements, to improve staff understanding and confidence.
Segregation
The segregation unit was now well managed. The number of prisoners held there had reduced considerably and the unit was rarely full. The regime had improved, with prisoners routinely able to attend work or activities off the unit, subject to individual risk assessment, an approach we rarely see elsewhere. Prisoners were also able to meet safety peer support mentors while on the unit, which supported reintegration.
The unit was of a good size and generally clean. All prisoners we spoke to reported positive treatment from staff, which was consistent with our observations.
Security
Expected outcomes: Security and good order are maintained through an attention to physical and procedural matters, including effective security intelligence and positive staff-prisoner relationships. Prisoners are safe from exposure to substance misuse and effective drug supply reduction measures are in place.
| HMIP prisoner survey | Yes | Compared with last inspection |
| In this prison, is it easy/very easy to get illicit drugs? | 43% | Higher |
| In this prison, is it easy/very easy to get alcohol? | 25% | Higher |
Security arrangements were generally proportionate and enabling, which supported improvements in culture and behaviour. However, illicit drug use remained a serious concern. Twenty‑five per cent of prisoners had tested positive in random mandatory drug tests over the past year, and there had been two drug‑related deaths since the previous inspection.
Efforts to tackle drug supply were hindered by limited investment in security infrastructure from HMPPS, some weak procedural processes, damaged equipment and less consistent use of the body scanner for new arrivals than we usually see elsewhere. Despite regular security meetings, it was not always clear how intelligence informed action to address identified risks.
The ISFL unit provided a supportive environment, and both prisoners and staff described it as having a strong sense of community. The joint meetings between safety, security and drug strategy teams (see Encouraging positive behaviour) were used to share intelligence and coordinate drug disruption activity, and intelligence‑led searches were frequent and productive. Arrangements to manage staff corruption were also effective.
The weekly review and response meeting provided good oversight of prisoners suspected to be under the influence of illicit substances. This included coordinated input from the safety team, access to drug services and, where appropriate, engagement in employment.
Safeguarding
Expected outcomes: The prison provides a safe environment which reduces the risk of self-harm and suicide. Prisoners at risk of self-harm or suicide are identified and given appropriate care and support. All vulnerable adults are identified, protected from harm and neglect and receive effective care and support.
Suicide and self-harm prevention
Since the previous inspection, there had been three deaths in custody, two linked to illicit drug use and one that the Prisons and Probation Ombudsman (PPO) had classified as non‑natural.
Recommendations arising from PPO investigations, mainly relating to emergency response procedures, had been implemented and these were subject to regular review.
Levels of self‑harm had increased by 29% since the previous inspection, and rates over the past 12 months were higher than in many similar prisons. There had been 24 incidents needing hospital treatment. However, serious self‑harm incidents were not routinely investigated, which limited learning.
| Data provided by the prison | |
| Annual self-harm rate per 1,000 prisoners in the 12 months prior to the inspection | 740 |
The weekly safety intervention meeting was well attended and provided a useful forum for coordinating specialist support for a small group of complex prisoners, who accounted for over half of all self‑harm incidents.
By contrast, the joint safety, security and drug strategy meeting (see Encouraging positive behaviour) generated very few actions relating to the reduction of self‑harm. Data and analysis were insufficient to understand trends or the drivers of self‑harm, which limited leaders’ ability to respond effectively and contributed to weaknesses in oversight.
Most assessment, care in custody and teamwork (ACCT) case management reviews for prisoners at risk of suicide or self-harm were completed promptly and attended by the mental health team. However, some sparse care plans and gaps in record keeping, compounded by the involvement of multiple case coordinators, undermined the consistency of care.
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Is it very/quite easy for you to speak to a Listener if you need to? | 61% | Higher |
The team of 11 Listeners (see Glossary) was supported by the safer custody team and the Samaritans. Additional provision from Unlock My Life (A peer‑led mental health and well-being project delivered in prisons across the UK, providing education and encouragement for prisoners to discuss mental health and its impact on them, and support one another.), mental health ambassadors and a self-help group run by the ‘pathways’ team (see also Mental health and Opportunities for prisoners to progress) further strengthened the overall support available.
Protection of adults at risk
Links with the adult safeguarding board were limited, and although there was a safeguarding strategy and referral process, most staff were unaware of them.
Section 3: Respect (Back to top)
Prisoners are treated with respect for their human dignity.
Staff/prisoner relationships
Expected outcomes: Prisoners are treated with respect by staff throughout their time in custody and are encouraged to take responsibility for their own actions and decisions.
Staff–prisoner relationships were generally positive, with more respondents to our survey than in similar prisons reporting respectful treatment and having someone to turn to. A ‘shout‑out board’ enabled staff and prisoners publicly to acknowledge good behaviour, which helped to promote and strengthen rapport.
Managers had focused on strengthening key work (see Glossary) and there were early signs of progress. In our survey, 83% of prisoners said that they had a key worker and 74%, more than in comparator prisons, found them helpful, and we found examples of good‑quality sessions in electronic case notes. However, delivery was not yet consistent or embedded, as acknowledged in the prison’s self assessment. Local performance data were unreliable, with some case notes incorrectly recorded as key work, and quality assurance failing to identify or address these discrepancies.
There were over 100 prisoner peer support and mentor roles, which helped prisoners feel part of a community, although many operated only during association and alongside other duties, limiting their impact. Red band prisoners (see Glossary) were used effectively across key functions such as the library and visits.
Daily life
Expected outcomes: Prisoners live in a clean and decent environment and are aware of the rules and routines of the prison. They are provided with essential basic services, are consulted regularly and can apply for additional services and assistance. The complaints and redress processes are efficient and fair.
Living conditions
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Are you in a cell on your own? | 100% | Higher |
| Can you have a shower every day if you want one? | 98% | Higher |
| Can you get cell cleaning materials every week if you want them? | 93% | Higher |
Despite the age of the prison, living conditions were good. Cells were appropriately equipped and in good decorative order, and many had been personalised.


Showers were reasonably clean, but some had drainage and ventilation problems.
Communal and outside areas were clean and well presented, with colour and wall art brightening the environment. Maintenance issues were resolved quickly, and smaller decorative jobs, such as cell painting, were managed by an officer-led prisoner works party.


Most wings had some cardiovascular equipment for prisoners to use throughout the day. Those on the ISFL unit benefited from a well-equipped on-wing gym and association room.

Access to clothing was one of the main frustrations for prisoners. To help prevent the ingress of drugs (see also Security), prisoners could not have clothes sent in by friends or family, and many could not afford to buy their own. Not all wings had adequate stocks of prison-issue clothing, and prisoners complained that items often went missing from the laundry, which leaders were attempting to address by improved oversight.
Residential services
The food served was of a reasonable quality and quantity. However, staff supervision of wing serveries was inadequate. Workers did not always wear correct personal protective equipment, serveries were not consistently clean, portion sizes were inconsistent and breakfast packs were not distributed fairly, with some prisoners reporting that they sometimes went without breakfast.
Cooking equipment and communal dining had been introduced on the wings since the previous inspection, and were welcomed by prisoners.
Shop arrangements were reasonable, but some prisoners from minority ethnic backgrounds told us that the range of goods did not meet their cultural or dietary preferences.
Prisoner consultation, applications and redress
There was good consultation with prisoners in council meetings, wing forums and at key committees, which led to improvements. However, outcomes were not always shared consistently, and further work was under way to strengthen communication and follow‑up.
The applications system was not operating effectively. Requests were poorly tracked and often untraceable, and prisoners often used the more organised complaints system as a substitute.
There were secure complaints boxes on each wing, with a clear collection process, and complaints were routinely reviewed to monitor trends, problems and outcomes. The most frequent complaints related to property parcels (see Living conditions) and the offender management unit (OMU; see Reducing reoffending).
A robust complaints quality assurance framework supported improvement through procedural justice work and regular reviews, providing consistent oversight and feedback to leaders.
Weekly legal visits were offered and prisoners had reasonable access to the library, where there was a suitable range of legal texts and Prison Service documents (see Time out of cell).
Fair treatment and inclusion
Expected outcomes: There is a clear approach to promoting equality of opportunity, eliminating unlawful discrimination and fostering good relationships. The distinct needs of prisoners with particular protected characteristics (see Glossary) or those who may be at risk of discrimination or unequal treatment, are recognised and addressed. Prisoners are able to practise their religion. The chaplaincy plays a full part in prison life and contributes to prisoners’ overall care, support and rehabilitation.
Oversight of work to promote fair treatment and inclusion had improved. Leaders had undertaken some limited consultation with prisoners from minority groups to understand their experiences. They had also used data to identify and investigate unfair treatment. This had led to prompt action to resolve specific issues, such as providing clothing covers to enable the searching of visitors whose religion prohibited direct contact with dogs, and the provision of fresh food for those following the Rastafarian Ital diet (see also Faith and religion).
However, some disparities persisted for prisoners from ethnic minority groups, including access to culturally relevant shop and library materials (see Residential services and Time out of cell).
There had been insufficient focus on improving longstanding negative outcomes for some groups, such as the poor engagement of young adults in purposeful activity and disproportionate levels of force used against neurodivergent prisoners.
Discrimination complaints were generally investigated thoroughly. However, responses were often slow, despite quality assurance measures.
Leaders had made promising connections with several external organisations to support some groups of prisoners, including the Gypsy, Roma and Traveller communities, and to host events such as a talk for Holocaust Memorial Day and a wheelchair basketball match.
Reasonable adjustments were generally made to enable prisoners with physical disabilities to participate in the regime, although these had sometimes taken too long to implement. Most wing staff we spoke to were aware of day‑to‑day support needs. However, access across parts of the site remained difficult for some prisoners with mobility problems, limiting their participation (see Strategy, clinical governance and partnerships).
Faith and religion
The well‑respected chaplaincy provided good faith and pastoral support and had made effective links with external faith groups. Although not all faith groups had a dedicated chaplain, prisoners were well supported in the interim. Support for Rastafarian prisoners was particularly strong, with joint working enabling access to an Ital diet and peer‑led weekly meetings.
Health, well-being and social care
Expected outcomes: Patients are cared for by services that assess and meet their health, social care and substance use needs and promote continuity of care on release. The standard of provision is similar to that which patients could expect to receive elsewhere in the community.
The inspection of health services was jointly undertaken by the Care Quality Commission (CQC) and HM Inspectorate of Prisons under a memorandum of understanding agreement between the agencies. The CQC found there were no breaches of the relevant regulations.
Strategy, clinical governance and partnerships
Central and North West London NHS Foundation Trust (‘CNWL’), supported by several partners, had improved performance across all key metrics since the previous inspection. A health needs analysis was under way to inform future commissioning, while staffing levels were stable and meeting demand.
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Do you think the overall quality of the health services here is very/quite good? | 56% | Higher |
Governance arrangements provided integrated, multi‑professional oversight of clinical practice, which was clearly demonstrated through meeting minutes and the risk register.
Learning from major incidents, including deaths in custody, was shared with clinicians through staff meetings and supervision, with audits checking that agreed actions had been implemented. The health care department had been refurbished, met infection control benchmarks and was clean and well maintained.
Some patients reported delays in responses to complaints. However, we found a proactive approach to resolving concerns face to face, supported by thoughtful written replies, and strengthened oversight was introduced during the inspection.
Mandatory training compliance was sound, with access to supervision and reflective practice, and most staff felt well supported. Clinical emergency preparedness was good, and staff had appropriate resuscitation skills. Out‑of‑hours support was provided by prison staff, although not all were aware of the location of automated external defibrillators or had received training in their use.
A newly appointed health care navigator was developing patient engagement, and prisoners valued regular face‑to‑face contact. Although some consultation activity had taken place, there were no peer networks or routine mechanisms to gather patient feedback.
There were no wing-based care facilities and some prisoners with mobility problems reported difficulties in accessing the health care department (see also Fair treatment and inclusion).
Promoting health and well-being
Health and well‑being events, delivered through effective partnership working, were viewed positively by patients who attended. The health care department lacked visible patient‑facing health information, including in other languages, although information displayed on the wings was better.
Disease prevention programmes were well managed, with ongoing initiatives to improve vaccine uptake, and patients could easily access NHS screening, health checks and sexual health services. However, there were no peer support health champions, which was a missed opportunity to support healthier living initiatives.
Primary care and inpatient services
There was strong clinical leadership of the primary care team, and staffing was stable, with vacancies filled and agency use significantly reduced.
New arrivals were screened by a nurse and received a secondary health screening the following day. Referrals were made promptly and medicines prescribed as necessary.
Primary care staff were available for extended hours on weekdays, with slightly reduced cover at weekends. A GP was on site three days a week and waiting times for routine appointments were reasonable. Prisoners could attend a daily nurse‑led drop‑in clinic and access a suitable range of services. However, waiting times for physiotherapy and podiatry were too long, at around 41 weeks.
Health care applications were paper based, collected daily during the week and triaged appropriately, with appointments booked with the relevant clinician. Staff had sufficient time to manage administrative work alongside clinical duties.
Care planning and record keeping were of a reasonable standard, with further developmental work planned. Care for patients with long‑term conditions was good, although education and support to promote self‑care were limited.
Administrative oversight of external hospital appointments was effective. However, there were too few prison officer escorts, resulting in delays to treatment and frequent same‑day cancellations
Social care
The memorandum of understanding between the prison, local authority and care provider had been reviewed and was waiting for ratification.
Primary care nurses screened prisoners for social care needs in reception. There had been no referrals for social care packages (see Glossary) in the previous 12 months. Few referrals for occupational therapy services had been made, but assessments were carried out promptly.
Despite the limited amount of social care activity, the prison and CNWL remained in regular contact with the local authority and made sure that social care remained a discussion topic at joint meetings.
Mental health
Responsive, psychologically informed care was provided through a Monday to Friday service. Initial screening and early contact with all new prisoners supported prompt identification of need. Referrals were reviewed by the multidisciplinary team, and urgent cases were usually seen on the same day by a small duty team of mental health nurses, including support for prisoners on an ACCT.
Partnership working with the prison was strong, with multidisciplinary collaboration, including with the specialist ‘pathways’ team (part of the offender personality disorder network), which provided impressive support for around 40 prisoners.
A highly skilled core team delivered a wide range of individual and group interventions. However, the purpose‑built group space within the team’s base was not accessible to patients, limiting the amount of group work available. Waiting times for interventions, including specialist support, were reasonable. Fifty‑nine patients were on the caseload, including 11 with severe and enduring mental ill‑health, who received comprehensive support; care plans showed regular contact and good detail. There were delays in accessing attention-deficit hyperactivity disorder and autism assessments, although the team was working through the backlog.
No patients had been transferred under the Mental Health Act in the past year. Few prisoners were released directly into the community, but arrangements and communication for any ongoing support were evident.
Support and treatment for prisoners with addictions and those who misuse substances
Leadership of clinical and psychosocial services was robust and supported effective delivery. Patients we spoke to were positive about the support provided. Partnership working was good and the team contributed consistently to drug strategy meetings.
All patients were seen on induction and those needing support were assessed within five days. Patients received harm minimisation advice and one-to-one input through several programmes and interventions.
There were 75 patients on the psychosocial services caseload, of whom nine were on opiate substitution therapy (OST). Reviews were regular, and treatment and psychosocial input reflected national guidance.
Clinical management of OST was safe. However, only patients who were transferred in on an existing prescription had access to long-acting buprenorphine (an opiate substitution medication); the ability to implement this for all patients could have supported longer-term rehabilitation.
Hepatitis B immunisation status for patients on OST was checked and boosters were provided promptly when needed.
The ISFL unit was a more effective and better‑developed model than we usually see. The psychosocial team covered all wings and offered harm minimisation advice to everyone suspected of using illicit substances.
Medicines optimisation and pharmacy services
Pharmacy services were delivered by a skilled team, working collaboratively with health partners and prison officers. A prescribing pharmacist ran clinics, clinically screened prescriptions and completed medicines reviews. Prescribing of potentially misused medicines was monitored closely, and a health care navigator supported patients with medicines information and clinic appointments.
Medicines administration was supported by pharmacy technicians, with prison officers supervising part of the queue. However, limited visibility in part of the administration area reduced privacy and increased the risk of diversion.
Medicines were supplied promptly from an external pharmacy; these were labelled and stored correctly, and transported safely around the prison. Repeat prescriptions were ordered two weeks in advance, and SystmOne (the electronic clinical record) was used effectively to record prescribing, administration and non‑attendance. Patients who did not present for critical medicines were followed up appropriately.
Many patients received medicines in possession (IP) following risk assessments, which were reviewed at least annually, or sooner if concerns arose. Compliance packs were provided where needed, and an automated collection point on one wing enabled some patients to collect IP medicines directly. Pharmacy technicians carried out random cell checks, with IP status reviewed when non‑compliance was identified.
Medicines, including over‑the‑counter products such as paracetamol, were available when the pharmacy was closed. However, medicines stock storage was untidy, which increased the risk of selection errors. Advance notice of court attendance, release or transfer enabled medicines to be prepared in a timely way.
Governance and oversight arrangements were good. Medicines errors were investigated, with actions taken to reduce recurrence; drug safety alerts were managed appropriately; and confidential and medicines waste were well managed.
Dental services and oral health
Time for Teeth provided six dental sessions per fortnight (two in one week and four the next). The dental team had worked hard to reduce waiting times for routine appointments and treatment, and these were now reasonable.
Urgent need was prioritised, with the dentist seeing additional patients when acute issues arose. The dental nurse visited the wings to provide oral health advice and appointment reminders, in order to reduce ‘did not attend’ rates. Prisoners were familiar with the dental nurse, which helped build relationships and improve communication.
Equipment was well maintained and serviced regularly. The dental suite was clean and met infection control standards, with a well‑ordered separate decontamination room. Staff received appropriate training and professional development.
Section 4: Purposeful activity (Back to top)
Prisoners are able and expected to engage in activity that is likely to benefit them.
Time out of cell
Expected outcomes: All prisoners have sufficient time out of cell (see Glossary) and are encouraged to engage in recreational and social activities which support their well-being and promote effective rehabilitation.
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Do you know what the unlock and lock-up times are supposed to be here? | 98% | Higher |
| For those who know what the unlock and lock-up times are supposed to be: Are these times usually kept to? | 81% | Higher |
| Do you usually spend less than 2 hours out of your cell each day on Monday to Fridays? | 1% | Lower |
Prisoners reported regular access to domestic time, fresh air and evening association, including at weekends. Time out of cell on the ISFL unit was even better, with prisoners unlocked throughout the core day.
Unemployment had reduced to 9.5%, from 40% at the time of the previous inspection (see also Education, skills and work activities). Unemployed prisoners received between 3.5 and eight hours out of cell each day, part-time workers between four and five hours, and full-time workers around 9.5 hours.
Association was supported by good equipment on each wing, including pool and table tennis tables and gym equipment. Access to fresh air was increased from one to two one-hour sessions daily outside of the winter months.
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Can you go to the gym or play sports more than three times a week? | 55% | Higher |
PE provision had improved and prisoners no longer had to choose between going to the gym and attending education or work. A broader range of classes, alongside well‑maintained facilities and recent investment in equipment, had increased attendance.


The programme included diverse sports sessions, specialist groups, joint staff–prisoner activities and strong involvement from external agencies, alongside a small number of accredited courses.
| HMIP prisoner survey | Yes | Compared with similar prisons |
| Are you able to visit the library once a week or more? | 80% | Higher |
A varied timetable enabled regular library access across the wings, education classes and workshops. Red band support ensured access for segregated and self‑isolating prisoners. A suitable range of materials was available.

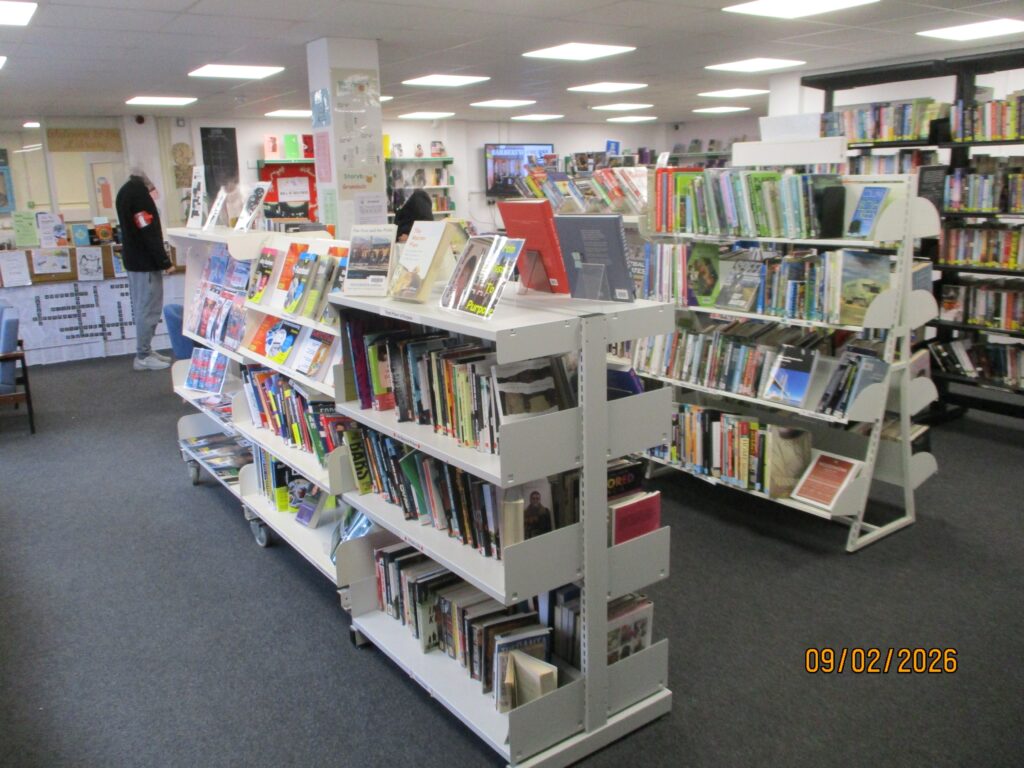

There were positive reading initiatives, including lower-level reading groups and Shannon Trust support (see Glossary), but prisoners from ethnic minority groups were not always able to access culturally relevant reading materials.
Education, skills and work activities
Ofsted inspects the provision of education, skills and work in custodial establishments in England. The following summary has been provided by Ofsted inspectors who attended this inspection. Their full report is published under ‘Further resources’.
Ofsted made the following assessments about the education, skills and work provision:
- Overall effectiveness: Requires improvement
- Quality of education: Requires improvement
- Behaviour and attitudes: Requires improvement
- Personal development: Requires improvement
- Leadership and management: Requires improvement
Leaders had a clear vision for their future education, skills and work (ESW) curriculum. However, the current curriculum did not meet the needs of enough prisoners by aligning with their interests or career aspirations. Although improved from the previous inspection, where inspectors found provision to be inadequate, the quality of the ESW provision was still not good enough.
A large percentage of prisoners were employed in full-time activity, with the remainder in part-time roles. The proportion of prisoners who were unemployed was low. Those not employed were generally either new to the prison or unfit for work. There were sufficient spaces for prisoners.
Milton Keynes College delivered education services, providing high‑quality teaching in a small number of subjects, including catering and business. In business, teachers helped prisoners develop a deeper understanding of the subject, challenging them effectively on their proposals, including the realities of revenue and market competition.
The small number of prisoners undertaking distance learning programmes received good‑quality, ongoing support and studied a wide range of subjects aligned to their individual interests, including A levels and bachelor’s degrees. Prisoners had sufficient access to study materials, and a few were able to use laptops for their learning. The virtual campus (see Glossary) had been replaced with an online learning package that was being phased in.
Instructors generally used verbal instructions and demonstration well. Prisoners produced items in woodwork, such as coat pegs, that were of the expected standard. However, too many did not value the work given to them and were unclear what technical knowledge they were expected to learn.
Although leaders had improved many aspects of reading across the prison, including new reading areas and the purchase of more contemporary literature, too many prisoners who needed support to improve their reading did not receive it. Prison-wide training for instructors and wing staff had been postponed.
For too many prisoners, there was insufficient work to keep them fully occupied, such as in the laundry. Leaders rightly recognised that the proportion of wing workers was too high and had plans to reduce the number of prisoners employed as cleaners and barbers. However, at the time of the inspection, these plans had not yet come into effect.
Leaders had well-developed plans to implement a range of new provision to replace the previous vocational curriculum. Current plans included a new barber shop, supermarket, café and art studio. However, at the time of the inspection, the provision was still months from opening.
Mostly, prisoners with an identified learning need received appropriate and helpful support in lessons. For example, staff used different reading aids to support prisoners with visual impairments, helping reduce fatigue during studies. However, support arrangements were often not implemented swiftly enough.
During induction, prisoners received suitable initial advice and guidance about the ESW opportunities available in the prison. However, the ongoing careers advice and guidance was not good enough. Information about employment pathways was confusing and not well enough related to prisoners’ future career ambitions.
Attendance at ESW activities varied significantly. Although much improved in the past year, there were too many instances where only a few, or no, prisoners attended their planned education, vocational training or work activities.
Leaders had introduced many enrichment activities for prisoners, including sports competitions. On the wings, prisoners had access to board games and leisure activities. However, many prisoners that inspectors spoke to were unaware of the breadth of such opportunities or had not participated in them.
Most prisoners did not understand well enough the risks related to radicalisation and extremism. While staff provided them with basic information about topics such as the ‘Prevent’ duty at induction, they did not revisit those topics sufficiently well.
Section 5: Preparation for release (Back to top)
Preparation for release is understood as a core function of the prison. Prisoners are supported to maintain and develop relationships with their family and friends. Prisoners are helped to reduce their likelihood of reoffending and their risk of harm is managed effectively. Prisoners are prepared for their release back into the community.
Children and families and contact with the outside world
Expected outcomes: The prison understands the importance of family ties to resettlement and reducing the risk of reoffending. The prison promotes and supports prisoners’ contact with their families and friends. Programmes aimed at developing parenting and relationship skills are facilitated by the prison. Prisoners not receiving visits are supported in other ways to establish or maintain family support.
The visits hall was small but clean, welcoming and well presented. Sessions were supported by the Prison Advice and Care Trust (PACT), which provided games to encourage positive family interaction, and visitors valued the introduction of Polaroid photographs which enabled families to take away a photo from their visit. Two‑hour afternoon sessions were available on Mondays, Tuesdays, Thursdays and at weekends, but the absence of evening visits limited flexibility for some families.
Refreshments were limited to cold snacks and cash payments, although during the inspection a hot item was added to the menu and card payments were introduced. Previous delays to the start of visits in the main hall had been resolved by deploying additional staff at lunchtime.
An impressive accessible visits room was well used and provided a calm, private environment for vulnerable visitors, including those with serious illness or physical disabilities. However, its private location away from the main visits hall meant that sessions routinely began up to 30 minutes late.
There was good oversight of prisoners who did not receive visits, with 125 identified at the time of the inspection. PACT delivered dedicated sessions six times a year, offering structured activities such as bingo, quizzes and competitions. Secure social video calling (see Glossary) was available but underused, with only three of the four booths operational.
Monthly family days (see Glossary) provided extended contact, themed activities and opportunities to share a meal. However, wider support to help maintain family relationships, such as structured casework or parenting programmes, was underdeveloped. A family engagement worker had started in January 2026 but had not yet begun to deliver one‑to‑one support.
Reducing reoffending
Expected outcomes: Prisoners are helped to change behaviours that contribute to offending. Staff help prisoners to demonstrate their progress.
Since the previous inspection, the establishment had changed function to become an adult male training prison. All prisoners were serving long sentences, including life and indeterminate sentences for public protection (IPP, see Glossary).
Leaders recognised the importance of creating a rehabilitative environment that supported long‑term change, particularly given the complexity and length of sentences of those held at the prison. Despite this, some prisoners complained about being unable to complete their sentence plan, often directing their frustrations towards the OMU (see Prisoner consultation, applications and redress).
We found evidence of an environment and culture likely to support rehabilitation. Prisoners generally felt safe, the prison was clean and not cramped, staff–prisoner relationships were positive (see Staff-prisoner relationships) and prisoners had plenty of opportunity to socialise out of their cells. In our survey, more respondents than at the time of the previous inspection said that their experience at the prison had made them less likely to reoffend.
There was reasonable oversight of work to reduce reoffending, and leaders were developing some promising initiatives to improve outcomes in the future, such as the Phoenix unit (see Opportunities for prisoners to progress) and the ‘high street’, a working environment to improve the experience of prisoners and provide practical training and life skills.
How staff were supporting prisoners and managing risk
The move to an adult population had led to a marked increase in demand on the team, with POMs now completing regular categorisation reviews, a six‑fold rise in parole hearings, and spending significantly more time writing reports.
Around two-thirds of the population had been convicted of a violent offence, and many were eligible for management under multi-agency public protection arrangements (MAPPA) on release.
Telephone monitoring linked to public protection concerns was rarely used. Although POMs assured us that it was considered for all new prisoners, weaknesses in record keeping meant that it was not possible to confirm this.
Many prisoners waited too long for an initial sentence progression plan. At the time of the inspection, 30 had been waiting for more than three months, and some much longer, delaying work on targets to reduce risk.
To reduce demand on POMs, leaders had decided that initial sentence plans would be completed by an agency probation officer over the telephone. Some prisoners told us that they found this impersonal, and it limited opportunities for POMs to build relationships.
Completed plans were not always reviewed to make sure that they remained current. Only 69% of prisoners had had an assessment completed in the previous year, and some had not had one for several years. In our survey, only 72% of respondents said that they had a sentence plan, of whom just 59% said that staff were helping them to meet their targets.
Prisoners approaching parole hearings received good support from their POMs, but for most others contact was infrequent and often cursory. Nevertheless, we saw some good‑quality, one‑to‑one risk‑focused work delivered by POMs over several sessions.
Most prisoners did not receive regular motivation or encouragement from a named key worker, which could have mitigated frustrations about contact. Leaders had identified this as a priority for improvement.
Opportunities for prisoners to progress
The prison delivered all four levels of the accredited offending behaviour programme (OBP) Building Choices. It planned around 60 places over the next 12 months, prioritising prisoners in the final two years of their sentence or approaching parole.
However, some prisoners in the final five years of their sentence, including those potentially eligible for open conditions, had been told that they would not be supported for progression until they had completed the programme, despite waits of up to three years to access it.
We saw a few examples where POMs had not recommended prisoners for open conditions solely because they had not completed an OBP, even where there was other evidence of improved self-awareness and risk reduction, such as positive engagement with the prison.
Forensic psychology services provided bespoke one‑to‑one risk reduction work for a small number of prisoners who were unsuitable for group‑based OBPs.
The excellent ‘pathways’ service (see Suicide and self-harm prevention and Mental health) continued to provide intensive, multidisciplinary support for around 40 prisoners with an identified personality disorder, including therapy and work to develop living and social skills. Several complex prisoners who had previously struggled in custody had progressed well after engaging with the service, including achieving positive parole outcomes.
The Stoic course, delivered by PE staff, helped many prisoners manage aggression and improve well‑being, and some had also engaged in ‘The Difference’, delivered by the chaplaincy to support personal development. Many prisoners had gained new skills through activities such as peer supporter roles, although they often sought these opportunities themselves rather than being directed by staff.
In the previous year, almost 160 prisoners had been recommended for transfer to open conditions, and most had progressed promptly, although limited capacity in the south of England caused delays for some.
The newly opened Phoenix wing was a promising initiative to support prisoners serving IPP sentences.
Returning to the community
Expected outcomes: Prisoners’ specific reintegration needs are met through good multi-agency working to maximise the likelihood of successful resettlement on release.
The single worker from the Creating Future Opportunities (CFO) Evolution project supported all prisoners approaching release, providing ‘through-the-gate’ mentoring and referrals to a range of support services.
Data suggested that no prisoners had been released homeless in the previous year. During that time, almost half (45%) of all discharges had gone to an approved premises under licence conditions, while only 26% had returned to sustainable accommodation.
Section 6: About HMP Aylesbury (Back to top)
Category of the prison
HMP Aylesbury is a category C training prison.
Brief history
The prison was opened as a County Gaol in 1847 and served as such until 1890, when it became a women’s prison. Two new wings were added in 1902, serving initially as an Inebriates Centre and in the 1930s as a girls’ borstal. In 1959, the prison was converted to house adult male prisoners and in 1961 it changed again to house young male offenders aged between18 and 20. In 1989, Aylesbury was designated as a long-term young offender institution. The prison transitioned to a category C training prison in October 2022.
Population
- 370 prisoners were held at the time of the inspection. There was operational capacity for 402. (Figures provided by the prison.)
- 378 new prisoners received over the last year.
- 22 foreign national prisoners.
- 43% of prisoners from black and minority ethnic backgrounds.
- Around a quarter (26.5%) were aged 21–29, with the remainder aged 30 or above.
- 63 prisoners released into the community over the last 12 months.
- 75 prisoners receiving support for substance use.
Short description of residential units
A wing – general population
B wing – Academy wing
C wing – general population
D wing – Phoenix unit (IPP wing)
F wing – ISFL unit
G wing – induction unit
Segregation unit
Prison status (public/private)
Public
Key providers
Physical health provider: Central and Northwest London NHS Foundation Trust
Mental health provider: Central and Northwest London NHS Foundation Trust
Substance misuse treatment provider: Forward Trust
Dental health provider: Time for Teeth
Prison education framework provider: Milton Keynes College
Escort contractor: GeoAmey
Prison group director
Laura Sapwell
Name of governor/director and date in post
Kevin Marshall-Clarke (June 2024)
Changes of governor/director since the last inspection
Mark Allen, June 2020 – March 2024
Date of last inspection
Full inspection: 22 November – 9 December 2022
IRP: 29–31 August 2023
Progress on concerns from the last inspection (Back to top)
.At our last inspection, in 2022, we raised 15 concerns, five of which were about areas of priority concern.
At this inspection we found the following progress:
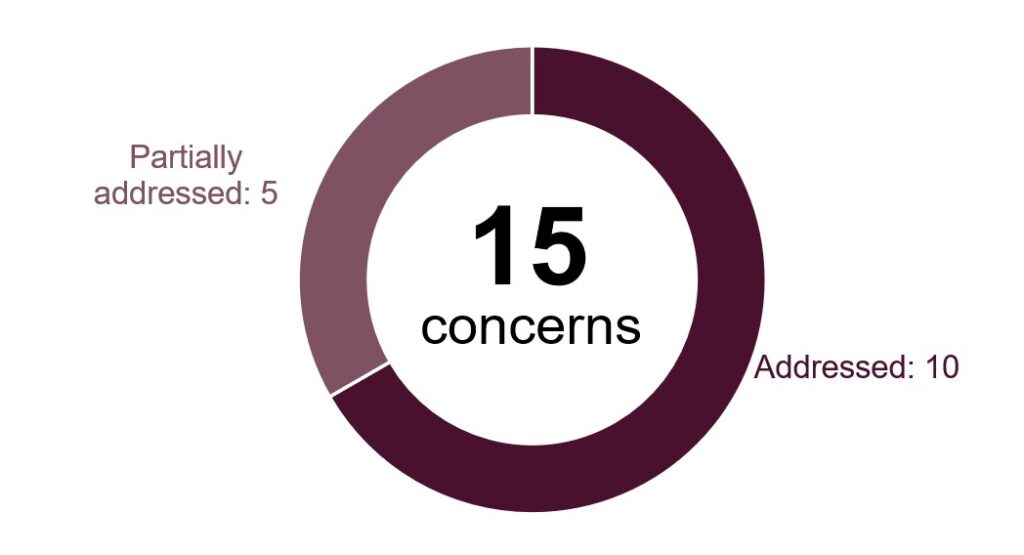
The following is a list of all the concerns raised, organised under the four tests of a healthy prison.
Safety
Priority concern
A shortage of staff in all grades and disciplines was limiting outcomes for prisoners. This included access to health care, time out of cell, education, skills and work and rehabilitation services.
Addressed
Key concerns
Levels of violence against staff and among prisoners were too high. The safety team was under-resourced and few incidents of violence were investigated.
Addressed
The incidence of use of force was too high, as was the use of the highest level of force such as PAVA incapacitant spray, batons and the body belt.
Addressed
Respect
Priority concern
There was a considerable shortage of suitably trained and experienced nursing and pharmacy staff. Patients’ routine or changing needs, including the management of long-term conditions, were not being assessed or met in a timely manner. This was creating serious risk.
Addressed
Key concern
Governance arrangements, including those for medicines management, were weak. Incident reporting was poor and risks to patient safety were not fully recorded or addressed.
Addressed
Work to promote equality was weak. Differences in treatment or access to the regime were not investigated or addressed.
Addressed
Purposeful activity
Priority concerns
Many prisoners spent less than one hour out of their cell each day. There was not enough education, training and work for the whole population to be meaningfully employed which was not good enough for a category C training prison.
Addressed
Leaders and managers did not use data effectively to evaluate the impact of the education, skills and work curriculum and drive improvements.
Partially addressed
Key concerns
Prisoners had very limited access to work or study. The planned six to seven hours a week was severely affected by poor attendance as prisoners prioritised other activities such as the gym.
Addressed
The provision of careers information, advice and guidance (CIAG) was inadequate. Too few prisoners benefited from high-quality, impartial CIAG and, as a result, too few prisoners had a planned learning pathway that prepared them for their future.
Partially addressed
Leaders had not prioritised reading in education. Leaders had not developed the curriculum to include reading as a distinct part of the education offer.
Partially addressed
Leaders had not ensured that prisoners completed appropriate training for their work roles. Prisoners did not work to industry standards. They did not receive appropriate training and, as a result, had not developed appropriate employment skills. Prisoners did not adhere to safe working practices, including wearing appropriate personal protective equipment in all work and vocational areas.
Partially addressed
Preparation for release
Priority concern
Aylesbury had been reroled to a category C training prison with inadequate planning or support. Work to reduce reoffending did not reflect the prison’s new population. Most of it still related to high risk, long-term young adults, who now made up only 23% of the population and would gradually leave altogether.
Addressed
Key concerns
There was too little support to help prisoners maintain or rebuild ties with their families and friends.
Addressed
The number of releases was increasing but no dedicated resettlement support was offered.
Partially addressed
More about this report (Back to top)
This report outlines the priority and key concerns from the inspection and our judgements against the four healthy prison tests. Each of the following four sections contains a detailed account of our findings against our Expectations for men’s prisons.
Find out more about our Expectations and how we inspect
Find out more about priority and key concerns
Find out about notable positive practice
Findings from the survey of prisoners and a detailed description of the survey methodology are published alongside this report. Please note that we only refer to comparisons with other comparable establishments or previous inspections when these are statistically significant. The significance level is set at 0.01, which means that there is only a 1% chance that the difference in results is due to chance.
The tables in this report which provide data from HMI Prisons prisoner surveys also include comparisons with similar prisons.
| Description | What it means |
| Lower | the prison’s percentage is statistically significantly lower than the comparator: prisons with the same function type, or at the last inspection |
| Higher | the prison’s percentage is statistically significantly higher than the comparator: prisons with the same function type, or at the last inspection |
| No difference | the prison’s percentage is not statistically significantly different to the comparator: prisons with the same function type, or at the last inspection |
Inspection team
This inspection was carried out by:
Angus Jones, Peer reviewer, on behalf of Chief Inspector
Ian Dickens, Team leader
Nadia Syed, Inspector
David Owens, Inspector
Lindsay Jones, Inspector
Dawn Mauldon, Inspector
Natalie Heeks, Inspector
Jasjeet Sohal, Researcher
Samantha Moses, Researcher
Emma King, Researcher
Stephen Eley, Lead health and social care inspector
Sarah Goodwin, Health and social care inspector
Helen Jackson, General Pharmaceutical Council inspector
Mathew Tedstone, Care Quality Commission inspector
Ian Frear, Lead Ofsted inspector
Saher Nijabat, Ofsted inspector
Cliff Shaw, Ofsted inspector
Further resources (Back to top)
These files may not be suitable for users of assistive technology.
Request an accessible format
If you use assistive technology (such as a screen reader) and need a version of any of these documents in a more accessible format, please email media@hmiprisons.gov.uk. Please tell us what format you need. It will help us if you say what assistive technology you use.
Find out more about the terms and abbreviations used in this report in our glossary.